

Translate this page into:
The impact of acupuncture on IVF success rates: A randomised controlled trial
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Clinical trials to assess the benefits of acupuncture on in vitro fertilisation (IVF) treatment have differed in study design, protocol, outcome measures and commercial bias. This heterogeneity has precluded any firm conclusion regarding the efficacy, or otherwise, of acupuncture in this field. To address this, 15 international acupuncturists with experience in treating women during IVF participated in Delphi questionnaires and reached a consensus protocol to be used in future research. We were among the first to adopt this newly agreed standard protocol. The aim of this study was to address whether the agreed acupuncture consensus protocol is beneficial for IVF outcomes and may be offered to women undergoing IVF.
Methods:
An randomised controlled trial, in which 157 women were randomised to receive either acupuncture treatment three times in the treatment cycle in addition to our standard IVF protocol (n = 79) or no acupuncture treatment (n = 78) in their first or second IVF cycle. They were between 23 and 43 years with body mass index below 30. The study group (n = 79) received acupuncture based on the Delphi consensus protocol, between days 6 and 8 of ovarian stimulation, and twice on the day of embryo transfer, before and after transfer. The IVF practitioner was blinded to the randomisation. The primary end point was live birth.
Results:
Fifteen out of 79 women in the intervention group withdrew from the study compared to 9/78 women from the control group (P < 0.001). A per-protocol analysis revealed that the rate of live births (27/64, 42% vs. 11/69, 15.94%, P = 0.001) and positive pregnancy tests (34/64, 53% vs. 19/69, 27.53%, P = 0.013) were significantly higher in the acupuncture group compared with the control group.
Conclusion:
The results of this study imply that acupuncture may be offered as a possible method of improving IVF outcome. This study followed a widely approved consensus protocol hoping to settle disagreement in the literature and resolve previous disparity.
Trial Registration: ClinicalTrials NCT02683967.
Keywords
acupuncture
IVF
live birth
pregnancy rate

BACKGROUND
Acupuncture is an ancient Chinese system of diagnosis and treatment which is said to help a variety of conditions including infertility. The delicate underlying mechanisms of acupuncture have been explained and described in the traditional Chinese medicine (TCM) language and in later years its possible physiological background has been repeatedly discussed.
There are increasing numbers of women reporting delays in conceiving. For the past 10 years, the number of assisted reproductive technology (ART) procedures has increased significantly despite the often great personal costs of ART. Over the last 2 decades, the use of acupuncture in female infertility as an adjuvant to conventional treatment in ART has been widely used. In vitro fertilisation (IVF) is associated with significant stress, which affects not only the outcome of the treatment but also the general well-being of the couple undergoing the procedure. There is a growing body of evidence that acupuncture reduces the stress of IVF and also improves its success rate.[1,2] The first clinical trial which suggested the efficacy of acupuncture in improving the clinical pregnancy rate in IVF was published in 1999.[3] In spite of dozens of clinical trials and reviews which aimed to assess investigating the benefits of acupuncture in various aspects of IVF, they all differ significantly in their study design, acupuncture timing, protocol and final outcome measures.[4,5,6]This lack of standardisation and extreme heterogeneity prevent us reaching a conclusion whether acupuncture is beneficial to IVF treatments, or otherwise, and should be offered to women undergoing IVF. For that reason, an adequately designed and conducted randomised controlled trial (RCT) in acupuncture is needed.
To address this, 15 international acupuncturists experienced in treating women with acupuncture during IVF participated in three rounds of Delphi questionnaires and reached a consensus for the use of TCM manual acupuncture, with 86% agreement. Such consensus offers guidance for further future research. We were among the first to adopt and use the consensus protocol. Recently, we were pleased to find out that a study[7] also realized the importance of a standard protocol and used the Delphi consensus in their trial. Our study presents a single-centre RCT and its aims and objectives were to compare acupuncture and IVF with IVF alone.
METHODS
The objective was to determine the clinical effectiveness of acupuncture in improving live birth and pregnancy rates in women undergoing IVF.
Study setting
This study was a single-centre RCT in a IVF centre of a public university. As our study was a part of the patient’s standard IVF care, the acupuncture sessions were performed at the fertility centre so as to accommodate the patient schedule.
Inclusion criteria
This included women under the age of 43 years with a body mass index < 30 undergoing their first or second IVF cycle (with a fresh or frozen/thawed embryo replacement).
Exclusion criteria
Women receiving donor eggs, body mass index ≥ 30 or currently having acupuncture or any other form of complementary and alternative medicine or having a contraindication to acupuncture, such as those with human immunodeficiency virus or hepatitis C positive, were excluded.
PATIENTS
Eligible couples were identified from the clinic database if they fulfilled the inclusion criteria. Written informed consent was obtained before randomisation. Ethical approval was given by a local ethics committee (13/LO/1356) and the trial was registered (NCT02683967).
Randomisation
Computer randomisation was performed by an independent worker in blocks of 10 and distributed in individual, consecutively numbered opaque envelopes immediately before the start of the IVF cycle following signed consent. Randomisation allocated couples to either the acupuncture group to receive acupuncture three times during the cycle of IVF (n = 79) or to the control group in which couples received only IVF but no acupuncture (n = 78) [Figure 1]. (To avoid disappointment, the patients randomised to the control group were offered three free acupuncture sessions to be used in a following IVF cycle should they be unsuccessful.)

- Consort diagram.
Power calculation
We anticipated a study participation rate of 50% of those eligible. On the basis of a predicted live birth rate of 20% in the controls and 40% in the acupuncture group, 79 patients were required in each group for a power of 80% and a significance level of P < 0.001.
Acupuncture protocol (based on Delphi consensus)
The first acupuncture treatment was manually administered between days 6 and 8 of the stimulated cycle in a style according to TCM. Chosen points during the stimulation phase include core points ST29, CV4, CV6, SP6, SP10 and up to five individualised additional points based on TCM pattern differentiation. Most of the point locations were mainly in the lower abdomen and some in the legs and hands (all performed bilaterally).
The duration of needling was approximately 25 minutes using disposable stainless-steel acupuncture needles (0.25 × 30 mm and 0.20 × 40 mm, Phoenix Medical, Chelmsford, UK). The needles were inserted to a depth varying from 10 ± 5 to 25 ± 5 mm at the acupoints depending on the location and patient’s physical figure. The practitioner (with 20 years of experience) maintained Deqi which is a needling sensation interpreted as a flow of Qi or the arrival of energy. This additional manual stimulation was performed during the initial treatment on days 6 to 8 and during the pre-embryo transfer treatment. The second and third treatments were performed on the day of embryo transfer − before and immediately after embryo transfer. Points used for pre-transfer included SP8, SP10, LR3, ST29, CV4 and one selected from HT7/PC6/YinTang (depending on presentation of women). Points used post-transfer included GV20, KD3, ST36, SP6 and PC6. Points Shenmen (auricular) and Zigong (lower abdomen) were used on the day of embryo transfer (ET).
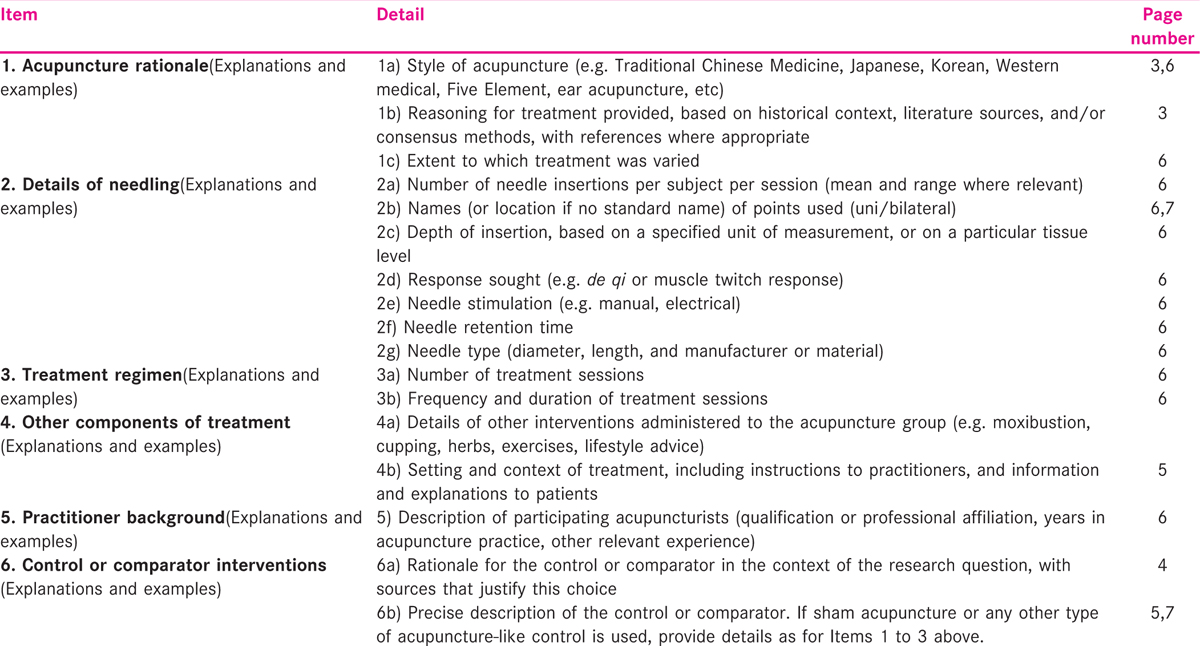
An acupuncture protocol describing the timing and acupoints for each session is stored with all acupuncture equipment so that the practitioner can check and ensure consistency and accuracy during the treatment. The checklist of the detailed information of the procedure is attached in Appendix 1.
Acupuncture points
Points on the innervations area to the uterus and ovaries in the abdominal muscles and in the leg were utilised as well as fertility defined points thought to improve blood circulation to the ovaries and the blood flow to the uterus and hence thought to improve follicular and endometrial responsiveness. Additional points were performed to manage stress.
IVF protocols
The IVF protocol that was used was decided by the attending clinician according to the departmental guidelines. Basically, predicted low and normal responders received long gonadotrophin releasing hormone (GnRH) agonist protocols with a starting follicle stimulating hormone (FSH) dose of 225 to 300 IU, whereas women predicted to be high responders received a GnRH antagonist protocol and a starting dose of FSH of 150 IU. Frozen/thawed embryos were replaced in an embryo replacement cycle applying the use of estradiol 2 mg three times daily and then vaginal progesterone starting the day before replacement.
Analysis
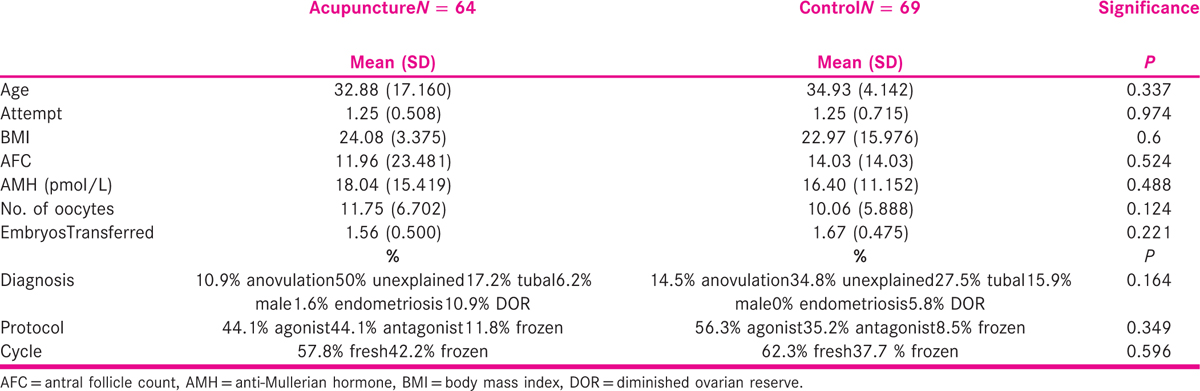
The results were analysed on an intention-to-treat (ITT) and per-protocol basis. The results were stratified according to age, duration of infertility, type of cycle (fresh or frozen), first or second IVF cycle and type of infertility [Table 1]. All results were faithfully recorded on a clinical research file designed especially for the purpose and, when completed, transferred to SPSS (Statistical Package for the Social Sciences, IBM SPSS Statistics).
Statistical analysis
A Chi-squared test and t-test were used to determine the differences between the acupuncture and control groups and compare the two arms of the study for both an ITT and per-protocol analysis. Chi-squared test was used for the secondary end points wherever applicable. As the dependent variables were categorical and not quantitative, we used these analysis methods.
RESULTS
One hundred fifty-seven women were randomly allocated to the intervention and the control groups. The intervention group (n = 79) was programmed for full acupuncture treatment, whereas the control group (n = 78) did not receive any acupuncture treatment. Either fresh or frozen/thawed embryo cycles were included. Of the 79 women allocated to the intervention group, 15 withdrew from the study (did not do the acupuncture treatment at all, did not finish the full treatment or had cancelled cycles), compared to nine women from the control group [Figure 1]. The number of dropouts in the acupuncture and the control group was significantly different (X2(1) = 12.67, P < 0.001). A set of Chi-square tests of independence was performed for both ITT and per-protocol analysis. The ITT analysis showed that rates of live birth 27/79 (34.60%) and positive pregnancy tests 35/79 (44.30%) were significantly higher in the acupuncture group compared to the control group in which rates of live birth were 11/78 (14.10%) and rates of positive pregnancy tests were 19/78 (24.36%), P < 0.001.
After excluding the dropouts from each group, a set of Chi-square tests of independence was performed to examine any differences between the acupuncture and the control groups (per protocol) regarding basal parameters [Table 1] and rates of live births, miscarriages and positive pregnancy tests [Table 2]. The rates of live births (X2 (1) = 11.207, P = 0 .001) and positive pregnancy tests (X2 (1) = 6.237, P = 0.013) were found to be significantly higher in the acupuncture group compared to the control group [Table 2]. No statistically significant difference was found between the groups in the miscarriage rates. There were no significant differences in the results of fresh and frozen cycles.
Safety and adverse effects
Acupuncture was performed based on professional standards of practice using disposable needles. There were no adverse events; on the contrary, patients from the acupuncture group filled a quality-of-life questionnaire and reported better quality of life and relief from the IVF symptoms after they had had the acupuncture sessions.
DISCUSSION
In this study, we have shown that rates of live birth and positive pregnancy tests are significantly higher following a consensus acupuncture protocol for women undergoing IVF treatment compared with a control group.
Acupuncture has been extensively studied to examine its effect on live birth and pregnancy rates. However, debate continues as different studies have used different protocols and their outcomes are contradictory. Hence, even with such extensive literature, no definitive conclusions regarding the value of acupuncture for IVF can be made. Analysing all studies so far with live birth as the primary outcome, different timings of acupuncture could be identified. One of the first RCTs was published in 1999 suggesting that acupuncture improved the clinical pregnancy rate in IVF.[3] In this study, 157 women undergoing IVF were randomised to acupuncture or controls before oocyte retrieval and a significantly higher pregnancy rate was observed in the acupuncture group. Since the RCT by Paulus et al.,[8] in which 25 minutes of acupuncture was performed before and after embryo transfer with improved pregnancy rates in the acupuncture group, several RCTs[9,10,11,12,13,14] and observational studies[15,16] have been conducted to assess the effect of acupuncture on live birth when applied around the time of embryo transfer. However, the results have been highly contradictory. While some RCTs showed improved pregnancy rates,[10,13,14] others showed no difference between the acupuncture and the control groups.[9,11,12] Another RCT divided women <40 years undergoing IVF/intracytoplasmic sperm injection into two groups and performed acupuncture in one group in three sessions (each lasting for 25 minutes), with the first session of 5 to 7 days before oocyte aspiration, second session of 2 to 3 days before egg retrieval and third session shortly after embryo transfer. The control group had no intervention. The number of women recruited in this preliminary study was limited; however, they concluded that their results did not support a positive effect of acupuncture on IVF.[17] Another negative RCT randomised 228 women into an acupuncture group where they received acupuncture on day 9 of ovarian stimulation, before and after embryo transfer and a placebo group with non-invasive sham acupuncture. They could not show any significant difference in the pregnancy rates between the two groups.[18]
Assessing subjective outcome like pain, anxiety and general well-being, normally suggests the use of appropriate placebo controls as otherwise the results may be biased by the women’s pre-judgement about the effect of acupuncture. However, while assessing objective outcomes like pregnancy rates, they are unlikely to be affected by the woman’s expectations and hence use of placebo control is questioned.[19] Furthermore, the method of non-penetrating needle technique (Streitberger) cannot be considered as a placebo as it has an acupressure effect, hence one must remember that ‘inert’ placebos are not inert and the validity of such trials is questionable.[18] After due consideration and heeding the advice of Manheimer,[19] we decided that no placebo should be employed and a control arm of no additional treatment would provide the most reliable results.
Controversial evidence is available for the use of acupuncture in the luteal phase of IVF. Although one RCT with 225 women supported use of acupuncture in the luteal phase to improve pregnancy rate,[20] another systematic review showed no benefits and suggested that luteal phase acupuncture should not be offered until further evidence is obtained.[5]
Does acupuncture improve live birth in IVF?
A recent systematic review and meta-analysis of 24 trials with 5807 participants has shown that although the pooled clinical pregnancy rates were higher in the acupuncture group, the live birth rates were not significantly different than the control group.[4] However, the live birth rates were found to be higher with acupuncture when the studies using Streitberger controls were excluded. Further differences were seen when different timings of acupuncture were analysed.
They concluded that acupuncture around the time of oocyte aspiration or controlled ovarian hyper-stimulation might be more effective in improving the pregnancy outcome in IVF.[4] This meta-analysis was recently re-evaluated in view of the marked heterogeneity. After removing a few trials, no significant benefit of acupuncture could be shown.[21] Also another systematic review in 2012 analysed 17 trials and showed no significant difference in clinical pregnancy, biochemical pregnancy, ongoing pregnancy or live birth rate between the acupuncture and the control groups.[22]
Hence, the evidence regarding the efficacy of acupuncture to improve clinical pregnancy rates is controversial. In spite of 40 clinical trials and nine systematic reviews, the debate still continues.
Problem with protocols used in different studies
As the effect of acupuncture differs along the menstrual cycle, acupuncture applied at different time points produces different results. Hence, different studies using acupuncture at different time points are likely to produce different effects and are not comparable. Even slight alteration in the regimen might produce significant changes in the results. Although some trials have used acupuncture only around oocyte aspiration[3] or around embryo transfer,[9,10,11,12,13,14] some have used it at different time points throughout the IVF treatment including ovarian stimulation, oocyte aspiration and embryo transfer.[17,18] Significant differences are noted not only in the timing but also in the acupuncture points used in the different studies. Therefore, it has been agreed that the quality of clinical acupuncture studies is moderate, suffers from lack of standardisation and extreme heterogeneity and that an adequately designed and conducted RCT in acupuncture is needed.[24] For that reason, this RCT is important as it is among the first to follow such an appropriately designed protocol which was achieved as an agreed consensus by experts in that field. The importance of using this newly derived consensus protocol is to be able to establish evidence based data and settle disagreement in the literature to resolve previous disparity. We believe this is the strength of this RCT. A limitation of the present study is the analysis of a relatively small group.
CONCLUSION
We have shown that using the acupuncture consensus protocol in women undergoing IVF has a positive effect on IVF outcome. This RCT is among the first studies to follow the agreed protocol and has demonstrated the positive effect of acupuncture on IVF success rates. Therefore, we suggest that acupuncture may be offered to women undergoing IVF treatments in an attempt to improve their treatment outcome. More studies following this consensus protocol are required in future to verify its results.
Financial support and sponsorship
None.Conflicts on interest
There are no conflicts of interest.
REFERENCES
- Building resilience: A preliminary exploration of women’s perceptions of the use of acupuncture as an adjunct to in vitro fertilisation. BMC Complement Altern Med. 2009;9:50.
- [Google Scholar]
- An exploratory study of the effect of acupuncture on self-efficacy for women seeking fertility support. Explore. 2010;6:330-4.
- [Google Scholar]
- A prospective randomised study of electro-acupuncture versus alfentanil as anesthesia during oocyte aspiration in in-vitro fertilization. Hum Reprod. 1999;14:2480-4.
- [Google Scholar]
- The effects of acupuncture on the pregnancy rates in women undergoing in vitro fertilization: A systematic review and meta-analysis. Fertil Steril. 2012;97:599-611.
- [Google Scholar]
- Acupuncture in IVF: A review of current literature. J Obstet Gynaecol. 2014;34:555-61.
- [Google Scholar]
- Effects of a Delphi consensus acupuncture treatment protocol on the levels of stress and vascular tone in women undergoing in-vitro fertilization: A randomized clinical trial protocol. BMC Complement AlternMed. 2017;17:197-205.
- [Google Scholar]
- Influence of acupuncture on the pregnancy rate in patients who undergo assisted reproduction therapy. Fertil Steril. 2002;77:721-4.
- [Google Scholar]
- Acupuncture on the day of embryo transfer: A randomised controlled trial of 635 patients. Reprod Biomed Online. 2010;21:366-72.
- [Google Scholar]
- The impact of acupuncture on in vitro fertilization outcome. Fertil Steril. 2009;91:723-6.
- [Google Scholar]
- Randomized controlled trial: Effects of acupuncture on pregnancy rates in women undergoing in vitro fertilization. Fertil Steril. 2011;95:583-7.
- [Google Scholar]
- Effect of acupuncture on rates of pregnancy among women undergoing in vitro fertilization. Fertil Steril. 2010;94(Suppl1):S170.
- [Google Scholar]
- Acupuncture on the day of embryo transfer significantly improves the reproductive outcome in infertile women: A prospective randomised trial. Fertil Steril. 2006;85:1341-6.
- [Google Scholar]
- Acupuncture improves IVF pregnancy rate in older women. Eur J Integrat Med. 2012;4:1876.
- [Google Scholar]
- Effect of acupuncture on assisted reproduction treatment outcomes. Acupunct Med. 2010;28 doi:10.1136/aim.2009.002022
- [Google Scholar]
- The role of acupuncture in ART: Preliminary results of an ongoing prospective randomised study. Hum Reprod. 2011;26:i230.
- [Google Scholar]
- Influence of acupuncture stimulation on pregnancy rates for women undergoing embryo transfer. Fertil Steril. 2006;85:1352-8.
- [Google Scholar]
- Selecting a control for in vitro fertilisation and acupuncture randomised controlled trials (RCTs): How sham controls may unnecessarily complicate the RCT evidence base. Fertil Steril. 2011;95:2456-61.
- [Google Scholar]
- Effect of acupuncture on the outcome of in vitro fertilisation and intracytoplasmic sperm injection: A randomised, prospective, controlled clinical study. Fertil Steril. 2006;85:1347-51.
- [Google Scholar]
- Effects of acupuncture on the outcomes of in vitro fertilisation: A systematic review and meta-analysis. J Altern Complement Med. 2012;18:429-39.
- [Google Scholar]
- Acupuncture improves in vitro fertilization live birth outcomes: A retrospective chart review. J Altern Complement Med. 2013;19:637-643. doi:10.1089/acm.2011.0888. Epub 2013 Jan 30
- [Google Scholar]
- Using a Delphi consensus process to develop an acupuncture treatment protocol by consensus for women undergoing Assisted Reproductive Technology treatment. BMC Complement Altern Med. 2012;12:88.
- [Google Scholar]




