

Translate this page into:
A prospective study to assess the mental health and quality of life in women undergoing assisted reproduction
Address for correspondence: Dr. Sudha Prasad, Bungalow No. 02, New Moti Bagh, Shanti Path, New Delhi 110021, India. E-mail: drsprasad@yahoo.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
Infertile women may experience high levels of psychological distress. The assessment of stress levels specifically related to infertility and the quality of life during infertility management needs to be evaluated.
Aims:
To study the psychological health of women undergoing assisted reproduction.
Settings and Design:
A cross-sectional study conducted between March 2014 and April 2015 at a tertiary care in-vitro fertilization setup in India.
Subjects and Methods:
Clinical interview and self-report measures were applied for an assessment of the psychological state of infertile women (N = 186). Anxiety was evaluated by Hamilton’s Rating Scale and Sinha’s Comprehensive Anxiety Test. Depression was assessed using Hamilton’s Rating Scale, Amritsar Depressive Inventory. Fertility and Quality of Life Questionnaire (FertiQoL) was applied to measure infertility specific stress. Overall life stress, covering all areas of life, was assessed using Presumptive Stressful Life Events Scale. Cornell Medical Index was applied to evaluate overall physical and mental health.
Statistical Analysis:
Student’s t-test and chi-square test were applied, and statistical significant levels were calculated at P < 0.05.
Results:
Clinically, significant depression was identified in 60.11–64.86% of the women. However, relatively lesser frequency of anxiety (27–37%) was observed. FertiQoL scores suggest that infertility treatment in itself is stressful, and nearly 80% of women reported increased levels of general life stresses.
Conclusion:
Being infertile has profound detrimental psychological impact on the life of women. Women undergoing treatment had significant high levels of psychological stress, depression and anxiety along with a lowered quality of life.
Keywords
Anxiety
depression
infertility
in-vitro fertilization and mental health

INTRODUCTION
The diagnostic confirmation and the management of infertility can have profound psychological impact.[1] Infertility affects personality that can be characterized by depression, increased anxiety, profound sadness, self-blame, social isolation, heightened interpersonal sensitivity and nearly 20% experiencing episodic suicidal ideation.[2,3]
Assisted reproductive technology (ART) procedures provide hope. However, the treatment methods are not only time consuming and expensive but these are having lower success rate (5–50%) also.[4] The stringent treatment regimen with uncertainty and prediction makes infertility management a very stressful process.[5] A very limited work was conducted specially in the Indian scenario in relation to the evaluation of the psychological impact of being infertile.[4,5]
The purpose of this study was to assess infertility-related psychological distress in women undergoing ART cycles.
SUBJECTS AND METHODS
Women seeking infertility management were recruited from the Outpatient Department of the Female Fertility & ART Clinic in a University Hospital tertiary care in-vitro fertilization (IVF) setup in North India. One-year prospective data of women who underwent assisted reproduction from March 2014 to April 2015 were evaluated to assess the impact of infertility on psychological health.
A total of 426 women were screened between March 2014 and April 2015, and among them, 207 women who underwent a first cycle of IVF treatment and satisfied the inclusion criteria were enrolled in the study. Among them, only 190 women were willing to undergo the assessment of psychological health. Moreover, 17 women refused to participate in the study, and four women were lost to follow-up due to incomplete treatment and or evaluation process. Finally, a total of 186 patients who underwent complete psychological evaluation and treatment cycles were included on the basis of criteria applied for the selection of women, which were as follows:
Inclusion criteria:
Age ≤38 years.
Infertility ≥2 year.
Women undergoing their first cycle of IVF treatment cycles.
Basal antral follicle count >5.
Baseline follicle-stimulating hormone (FSH) and luteinzing hormone (LH) ≤10 mIU/ml.
Baseline estradiol (E2) levels ≤50 pg/ml.
Normal serum prolactin and thyroid-stimulating hormone (TSH) levels.
Normal semen parameters as per World Health Organization (WHO) definition.[6]
Exclusion criteria:
Infertility attributed to endocrinal abnormalities.
Documented poor response in the previous ovarian stimulation.
Premature ovarian failure.
Severe male factor infertility.
Stage III and IV endometriosis.
Known psychological disorders.
Known medical disorders.
Women who did not complete psychological tests as in the study protocol.
Women who did not follow through with ART treatment.
Women worked up for repeat in vitro fertilization/intracytoplasmic sperm injection-embryo transfer (IVF/ICSI-ET) cycles.
Any referred patient (women) who has already undergone IVF/ICSI-ET cycle.
Ethical clearance was obtained from the Institution Ethics Committee of the college and associated hospitals to conduct the study. A written informed consent was taken after explaining the methodology, the possible associated risks, benefits and the side effects of the entire counseling and treatment cycle to the women/couple. Clinical interview (CI) and self-report measures (SRM) were applied for the assessment of the psychological state of women.
The psychological state of the infertile women who underwent assisted reproduction was evaluated qualitatively and quantitatively by the psychological tests and CI. To ensure a greater reliability and validity of the findings in relation to mental health, seven psychological tests were employed. Women who underwent IVF/ICSI-ET cycles were evaluated by Hamilton’s Rating Scale (HAM-A)[7] and Sinha’s Comprehensive Anxiety Test (SCAT) for measuring anxiety.[8] Hamilton’s Rating Scale (HAM-D),[9] Amritsar Depressive Inventory (ADI)[10] was used for measuring depression, Presumptive Stressful Life Events Scale (PSLES)[11] for general life stress and Fertility and Quality of Life Questionnaire (FertiQoL)[12,13] for the quality of life as affected by infertility and its treatment. Cornell Medical Index (CMI) gave an overall index of physical and mental health.[14]
Women attending the IVF & Reproductive Biology Centre were called for psychological assessment and counseling session. These psychological tests were applied to measure the stress levels in women who underwent IVF/ICSI-ET treatment cycles. In addition, qualitative data from individual counseling sessions was considered for evaluation. To ensure a greater reliability and validity of the findings, the assessment of mental health was performed by two methods. The methods are called as (a) CI and (b) SRM.
(a) CI: The CI was conducted to evaluate the qualitative and quantitative parameters (variables) of the affected individuals. It was achieved by applying three psychological tests, that is, HAM-A, HAM-D and PSLES.
(i) HAM-A: The HAM-A is a clinician rated evaluation. HAM-A measures both psychological anxiety (mental agitation, anxious mood, fear and psychological distress, etc.) and physical complaints, that is, somatic, muscular symptoms related to anxiety.[6] The scores of HAM-A are interpreted as follows:

(ii) HAM-D: The HAM-D is designed for adults to rate the severity of depression, the feeling of guilt, suicide ideation, insomnia, retardation, anxiety, weight loss and somatic symptoms.[9] The interpretation from HAM-D scores in relation to the level of depression is as follows:

(iii) PSLES: The PSLES is used to assess general life stress arising due to various life events, such as death, divorce, accident, etc. It contains a list of 51 parameters to measure various stressful life events that may contribute to illness. Normal Indian reproductive age group population experiences these events. The different life events with stress level rating and scores have been given in the questionnaire itself. The total scores give an index of the overall stress in the individual.[11] A high score creates a risk for illness in the person.
The interpretation of scores is as follows:

(b) SRM: The SRM was conducted by applying four psychological tests, namely, CMI, ADI, SCAT and FertiQoL.
(i) CMI: The CMI is a health questionnaire that identifies patients requiring general medical investigations. It is used for the epidemiological surveys of physical and mental health.[14] It contains two different sections. The first section deals with physical complaints and symptoms, while the second section deals with mood and feeling patterns. It includes mostly all the body organs such as eyes, ears, stomach, heart and their correlated symptoms such as nervous system, respiratory system, digestive tract, cardiovascular system, musculoskeletal system, genito-urinary system etc. Apart from this, it also includes psychological symptoms. Higher the rating, higher will be the stress levels. The standardized norms for the interpretation of scores have been given.
(ii) ADI: The ADI was initially developed in India for use in the Indian settings; it is currently also being used by NHS, UK for migrant Indian population requiring mental health services.[15] It contains 30 questions that evaluate the feelings of guilt, helplessness, hopelessness and worthlessness that characterize depression. In addition, included are the aches and pains that are expressed as the masked symptoms of depression. Higher the score on ADI, greater the level of depression.[10] Norms are given to categorize a person as having mild, moderate or severe depression.
(iii) SCAT: The SCAT gives an index of the anxiety levels in patients. It covers many aspects of life such as home, health and social and emotional features.[8] Higher the score, greater is the level of anxiety. Norms are given to classify the person as falling into mild, moderate or severe anxiety category.
(iv) FertiQoL: The FertiQoL is the first internationally validated psychological tool to measure the quality of life in individuals who are experiencing fertility problems. It contains the following two main sections: (i) Core FertiQoL and (ii) Treatment FertiQoL.[12,13]
The Core FertiQoL is the fertility quality of life across the Emotional, Mind–Body, Relational and Social subscales. The Emotional subscale score shows the impact of negative emotions (e.g., jealousy and resentment, sadness and depression) on the quality of life. The Mind–Body subscale score shows the impact of fertility problems on physical health (e.g., fatigue and pain), cognitions (e.g., concentration) and behavior (e.g., disrupted daily activities and delayed life plans). The Relational subscale score shows the impact of fertility problems on the marriage or partnership (e.g., sexuality, communication and commitment). The Social subscale score shows the extent to which social interactions have been affected by fertility problems (e.g., social inclusion, expectations, stigma and support).
The Treatment FertiQoL is the quality of life across the Treatment Environment and Treatment Tolerability. The Treatment Environment subscale score shows the extent to which the accessibility and quality of treatment impact the quality of life. The Treatment Tolerability subscale score shows the extent to which fertility medical services impact daily life.
The Total FertiQoL score is the quality of life for the Core and Treatment FertiQoL combined.
In this test, higher score denotes a better quality of life. Although no norms are given, the relative scores within the subsections of the FertiQoL are used to identify the area of life with relatively good quality and those aspects with poor quality.
Data were entered in a computerized database (spreadsheet). Statistical analysis was performed by Statistical Package for the Social Sciences software (version 21.0; SPSS S.L., Madrid, Spain). Data were checked for normality by using Shaipro–Wilk test prior to statistical analysis. All tests of statistical significance were two tailed. Data were presented as a number (%), mean ± standard deviation (SD) and median (range). The categorical variables were analyzed using the chi-square (χ2) and or Fisher’s exact test as appropriate. Statistical significant level were calculated at P < 0.05.
RESULTS
Efforts were made to study the mental health of infertile women who were seeking infertility management. Information regarding their economic status and other forms of social support was obtained using a semi-structured questionnaire, which was modified specially for infertile couples. Question and answer sessions for women were conducted consecutively by the counselor to obtain qualitative and quantitative data using CIs and SRMs. Mean scores and the frequency distribution of scores on each of the seven tests were used for descriptive and inferential analysis. Women’s subjective viewpoints and perceptions regarding their condition with its ongoing impact on their lives were noted for providing them therapeutic counseling.
Demographic data
The women in the study were between the ages of 21–38 years. The mean age of the women was 31.35 ± 4.10 years Table 1. The findings were evaluated and depicted in Table 1.

Women were categorized according to the duration of infertility. The duration of infertility ranged between 2 and 21 years, with the mean duration being 7.38 years. Eighty-seven percent women had less than 5 years of infertility, 10.64% had between 5 and 14 years and 1.60% had more than 15 years of infertility. The economical strata of the participants were also assessed, and it was found that for most of the women (82%), their family annual income was less than Rs. 500,000.
Psychological assessment
Overall physical and emotional health (Cornell Medical Index)
The mean score in our patients was close to the cutoff values for physical distress, psychological distress and total overall distress. This indicated that the group as a whole was close to being significantly distressed both physically and emotionally Table 1.
The frequency distribution below and above the cutoff values showed that nearly 34% of the women experienced significant levels of both physical health problems and emotional distress. It was observed that 31% of the women had significant levels of any physical component, whereas 36% (25) reported a significant degree of emotional distress. This included a feeling of inadequacy, depression, anxiety, sensitivity, anger and tension [Table 2].

Depression
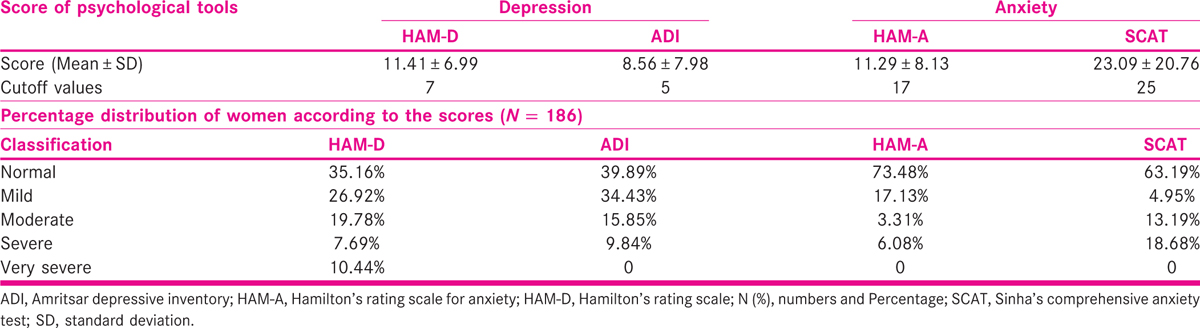
The HAM-D and the ADI were used to assess depression. Both the methods of assessment consistently showed similar outcomes. The mean scores on both ADI and HAM-D were above the cutoff values indicating the presence of clinically significant depression in the group as a whole. The frequency distribution of scores showed that a depression with a varying degree of severity, ranging from mild to very severe, was present in 60.11–64.86% of the women undergoing IVF treatment. Less than 40% of the women were normal [Table 3].
Anxiety
The scores of psychological tools applied for measuring the anxiety (HAM-A and SCAT) levels in infertile women were as follows. It was observed that mean values for anxiety were below the cutoff values in both HAM-A and SCAT. This showed that the group as a whole was not suffering from clinically significant anxiety. The frequency distribution of scores showed that 63.19–73.48% of the women did not experience anxiety or were normal. However, 9.39–31.87% of the women had moderate or severe anxiety level. Hence, although the majority of infertile women receiving treatment were not highly anxious, a small proportion were anxious, and their early identification during treatment will be helpful [Table 3].
General life stress
The mean score on PSLES in the women was higher than the cutoff values; hence, the overall life stress experienced by the group was much higher than a normal person, and made them prone to physical as well as psychological illness. The frequency distribution on the PSLES or general life stress scores showed that nearly 80% of women undergoing IVF treatment experienced many other life stresses because of infertility. The main sources of infertility-related general life stress were marital conflict, conflict with in-laws, family conflicts, financial problems, sexual problems and the prophecy of astrologers and palmists as depicted in Table 4.

Quality of life assessment with Fertility and Quality of Life Questionnaire
Impact of infertility on quality of life: Core FertiQoL scores: We noted that more than half of the women scored less than 50 in all four aspects namely Emotional, Mind–Body, Relational and Social aspects that reflected their poor quality of life. This meant that infertility lowered their quality of life significantly. The differences in score distribution in the four sections of the Core FertiQoL were statistically significant (P ≤ 0.0001) and showed that family and marriage counseling is mandatory to improve the psyche of women [Table 5].

The lowest mean scores were in the relational dimension, indicating that the maximum negative impact of infertility was on the sexual relations due to a reduced feeling of affection, intimacy or commitment, and an inability to communicate feelings related to infertility. The majority of women, nearly 60%, reported a relatively low quality of life in this dimension of the FertiQoL.
The emotional state of the women was also affected, though to a lesser extent, with nearly 55% experiencing negative emotions, for example, jealousy, resentment, sadness and depression that negatively affected the quality of life. The damage to mind/body and the social life was less compared to family and marital relations and emotions.
Impact of infertility treatment by ART on the quality of life: Treatment FertiQoL scores: The FertiQoL treatment scores showed a good ability to tolerate the treatment process, even though many women perceived treatment environment as less favorable. Both mean scores and the frequency distribution reveal the same [Table 6].
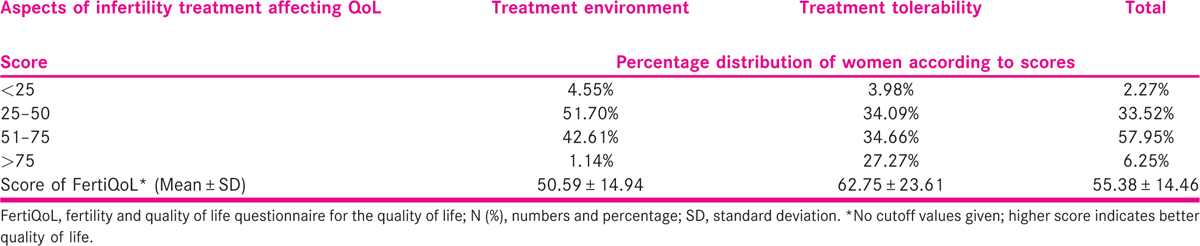
The frequency distribution of total scores indicated significantly lower total scores on core FertiQoL than total treatment FertiQoL scores (chi-square value core vs. treatment FertiQoL: 8.43, df: 3; P = 0.037).
Correlations of demographic variables with psychological test scores
The FertiQoL subscales showed correlation with age and education. The scores on the tolerability scale of the treatment FertiQoL negatively correlated with age (P = 0.037). Thus with increasing age, the treatment became less tolerable. Education showed significant (P = 0.046) positive correlation with the mind/body section of the core FertiQoL and the tolerability section of the treatment FertiQoL. This meant that, higher the education level, greater was the quality of life and better was the ability to deal with treatment and other life activities in general. The duration of illness and income did not show correlation with psychological test scores.
DISCUSSION
The stress of infertility and its treatment significantly increased depression in the women we studied. Anxiety, though present, was not so marked. The stress-induced psychological damage resulted in impaired relations with family members especially the husband. Majority, that is, 80% of these women, experienced a heightened overall life stress, which was high enough in magnitude to render them susceptible to a multitude of stress-induced diseases. The quality of life was reduced. Perhaps the two most relevant questions that this study seeks to answer are these:
Should psychological screening be a part of the infertility management process?
What areas of the woman’s life need to be addressed during the counseling process?
Should psychological screening be a part of the infertility management process?
The WHO in 1998 designed the quality of life as “individual’s perceptions to their positions in life in content of culture and value systems in which they live and in relation to their life’s goals, expectations, standards and concerns.” A poor quality of life is present in infertile women along with depression, anxiety or distress.
They should definitely acquire stress management skills prior to starting the infertility treatment. This is important for the following various reasons:
To improve treatment outcome: The negative subjective states induced by infertility and its management may have an impact on the subsequent fertility[16] and the success of treatment.[17] Boivin and Schmidt reported that infertility-induced stress was associated with a poorer treatment outcome in women and men, with the effect significantly more pronounced for women. The infertility-induced stress arising in the personal and marital domain showed greater associations with treatment outcome than did stress from the social domain.[18] The women who reported more marital distress required more treatment cycles to conceive than women reporting less marital distress.
To ensure treatment compliance and continuation: Studies in India as well as abroad have reported that a high percentage of couples discontinued the treatment due to psychological stress.[19] High scores on CMI have been the predictors of high dropout rate from the IVF treatment. Shinoda et al. noted that 60% of the patients belonging to high emotional distress discontinued treatment, and 90% of these gave up treatment within 6 months.[20] The negative emotions caused by infertility as well as its treatment influenced the willingness to continue with treatment,[21] treatment evaluation,[22] as well as the long-term satisfaction people can hope to achieve if treatment is unsuccessful and they remain childless[23] The chances of positive outcome increase, the longer the women stay in the treatment process. By discontinuing the treatment prematurely, their chances of ever having a child become remote.
To improve the quality of life: Psychosocial studies convincingly demonstrate that the negative reactions to infertility and its treatment[24] impact on the overall life satisfaction and well-being.[25] The quality of life is adversely affected. Studies have reported that infertility exerts pervasive negative effect on the quality of life, compromising planning and commitment to other life activities. The effect occurs in both men and women, but it is more so in women.[26] We need to screen the psychological ambience and the quality of life of all women planning to undergo infertility management so that they may acquire the skills necessary to face and cure infertility. The role of counseling and therapy here cannot be overstated; we should tailor it according to the woman and her requirements. Thus, psychological screening should be a definitive part of infertility management.
What areas of the woman’s life need to be addressed during the counseling process?
There are certain common trends and themes that can be useful and borne in mind when dealing with the infertile women. Our findings revealed that infertility caused more significant negative impact to the quality of life than its treatment by ART. The low FertiQoL scores in our patients show how counseling is mandatory to improve the psyche of women.
First, depression is the most commonly occurring emotional state in the infertile women undergoing ART and must be tackled by counseling. Grief reaction predominated in infertility due to the perception of many loses like; the loss of experience of pregnancy, childbirth, a loss of state of parenthood including the activities and relationships that it entails.
Secondly, an important finding of this study is that the primary family relations were most affected and relational dimension was worst hit because of poor quality of life and relationship. There are reduced feelings of affection, intimacy or commitment, and an inability to communicate feelings related to infertility with spouse and other significant members of the extended family.
Hence, counseling must aim to improve family relations with objectives of assassinating the depression, anxiety and feelings of isolation in women undergoing assisted reproduction. It is important to involve the spouse in the entire infertility management program right from the beginning. Relationship family and marriage counseling should involve the husband and the other significant members of the extended family such as the in-laws, so that there is a better communication and sharing of burden, and the myths and superstitions regarding infertility can be dispelled. In our cultural context, the woman faces the threat of divorce, even if the male factor is the primary cause of infertility.
Third important finding was a high positive correlation between education and the quality of life as well as with better treatment tolerability in this study. This indicates that the women in the lower educational strata need more psychological support, counseling and therapy to deal with the stress caused by infertility. In the women with lower education level, the professional choices are limited, and motherhood becomes the most important marker of their own self-identity. They find infertility especially difficult to accept and deal with. Other authors report similar findings.[27] In addition, lower education level decreased the tolerability toward the treatment process itself, probably due to difficulty in fully understanding the treatment procedure.
CONCLUSION
This study was conducted to assess the psychological impact as well as the mental health of infertile women undergoing IVF treatment at a public sector assisted reproduction clinic in India. The sentiments of being infertile have profound detrimental psychological impact on the life of women. It was observed that women undergoing treatment for their infertility had significant high levels of stress, depression and anxiety, along with a lowered quality of life. The high stress levels further increases the risk of illness. There is a need to identify the women who require psychological intervention along with regular ART treatment. Patient-tailored counseling corresponding to their educational status can help in achieving positive pregnancy outcome in women undergoing assisted reproduction. The optimistic attitude in marital relationship itself can salvage the compliance of treatment cycles as well.
Financial support and sponsorship
This study is supported by Indian Council of Medical Research (ICMR), New Delhi, India.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
The authors are grateful to the patients for participation and providing their consent to conduct this study. Assistance form the staff of IVF and Reproductive Biology Centre is also acknowledged.
REFERENCES
- Psychiatric morbidity in the infertile population: A reconceptualization. Fertil Steril. 1990;53:654-61.
- [Google Scholar]
- The experiences of couples who have had infertility treatment in the United Kingdom: Results of a survey performed in 1997. Hum Reprod. 1999;14:934-8.
- [Google Scholar]
- 2013. Assisted Reproductive Technology Success Rates: National Summary and Fertility Clinic Reports. Available from: http://www.cdc.gov/ART/PDF/ART2013_National_Summary_reprot.pdf.
- Psychosocial adjustment to infertility and its treatment: Male and female responses at different stages of IVF/ET treatment. J Psychosom Res. 1994;38:229-40.
- [Google Scholar]
- WHO Laboratory Manual for the Examination and Processing of Human Semen (5th). Geneva: WHO Press; 2010.
- Manual for Sinha’s Comprehensive Anxiety Test (SCAT). Agra: National Psychological Corporation; 1995.
- A new depressive inventory − Amritsar Depressive Inventory. Indian J Psychiatry. 1974;16:183-6.
- [Google Scholar]
- Presumptive Stressful Life Events Scale (PSLES) − A new stressful life events scale for use in India. Indian J Psychiatry. 1984;26:107-14.
- [Google Scholar]
- The fertility quality of life (FertiQoL) tool: Development and general psychometric properties. Hum Reprod. 2011;26:2084-91.
- [Google Scholar]
- Development and preliminary validation of the fertility quality of life (FertiQoL) tool. Fertil Steril. 2011;96:409-15.
- [Google Scholar]
- Cornell Medical Index Health Questionnaire − Hindi Translation. Chandigarh: Psychiatry Dept PGIMER; 1978.
- Cross-cultural validity of the Amritsar Depression Inventory and the General Health Questionnaire amongst English and Punjabi primary care attenders. Soc Psychiatry Psychiatr Epidemiol. 2000;35:248-54.
- [Google Scholar]
- Stress reduces conception probabilities across the fertile window: Evidence in support of relaxation. Fertil Steril. 2011;95:2184-9.
- [Google Scholar]
- Depression, anxiety and stress among infertile women and the impact of counseling on these levels. Innov J Med Health Sci. 2013;3:110-2.
- [Google Scholar]
- Infertility-related stress in men and women predicts treatment outcome 1 year later. Fertil Steril. 2005;83:1745-52.
- [Google Scholar]
- Why do couples discontinue in vitro fertilization treatment? A cohort study. Fertil Steril. 2004;81:258-61.
- [Google Scholar]
- Infertility patient’s mental health condition using the Cornell Medical Index (CMI) Fertil Steril. 2009;92:133-4.
- [Google Scholar]
- Reasons for dropout in an in vitro fertilization/intracytoplasmic sperm injection program. Fertil Steril. 2004;81:262-8.
- [Google Scholar]
- The patients’ perspective on fertility care: A systematic review. Hum Reprod Update. 2010;16:467-87.
- [Google Scholar]
- Reconstructing their lives: A longitudinal, qualitative analysis of the transition to biological childlessness for infertile couples. J Couns Dev. 2001;79:439-49.
- [Google Scholar]
- Women’s emotional adjustment to IVF: A systematic review of 25 years of research. Hum Reprod Update. 2007;13:27-36.
- [Google Scholar]
- Infertility and psychological distress: A critical review of the literature. Soc Sci Med. 1997;45:1679-704.
- [Google Scholar]
- Is fertility-problem stress different? The dynamics of stress in fertile and infertile couples. Fertil Steril. 1992;57:1247-53.
- [Google Scholar]
- Infertility and Assisted Reproduction − Mental Health Aspects of Women’s Reproductive Health: a global review of the literature. Geneva: World Health Organization; 2009. p. :128-46.




