Translate this page into:
Genital tuberculosis and infertility
Address for correspondence: Dr. Jai B. Sharma, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110029, India. E-mail: jbsharma2000@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Female genital tuberculosis (TB) is an important cause of significant morbidity, short- and long-term sequelae especially in infertility in which incidence varies from 5 to 15% cases in India. The causative agent is Mycobacterium tuberculosis. The fallopian tubes are mainly involved in 90 to 100% cases, endometrium in 60 to 80% cases, ovaries in 30% cases, and cervix in 15% cases of genital TB. Vagina and vulva TB is rare involving 1 to 2% cases. Diagnosis is made by detection of acid fast bacilli on microscopy or culture on endometrial biopsy or on histopathological detection of epithelioid granuloma on biopsy. Polymerase chain reaction (PCR) may be false positive and alone is not sufficient to make the diagnosis. Laparoscopy and hysteroscopy is the gold standard for the diagnosis of the disease. Treatment is by giving daily therapy of rifampicin (R), isoniazid (H), pyrazinamide (Z), and ethambutol (E) for 2 months followed by rifampicin (R) and isoniazid (H) daily for 4 months. Three weekly dosing throughout therapy (RHZE thrice weekly for 2 months followed by RH thrice weekly for 4 months) can be given as Directly Observed Treatment Short Course. Surgery is rarely required only for drainage of abscesses. Role of in vitro fertilization and embryo transfer is required in women whose fallopian tubes are damaged but endometrium is healthy. Surrogacy or adoption is needed for women whose endometrium is damaged.
Keywords
acid fast bacilli
genital tuberculosis
infertility
laparoscopy
polymerase chain reaction

INTRODUCTION
According to Global TB Report 2016, there were an estimated 10.4 million new tuberculosis (TB) cases worldwide (3.5 million in women), with 2 million deaths.[1] India has one of the highest incidences of TB in the world.[1,2] Over 95% of new TB cases and deaths occur in developing countries with 75% patients being in the most economically productive age group (15–54 years) causing great economic burden on the family and the nation.[2,3] There has been a 2 to 3-fold increase in TB cases in sub-Saharan Africa due to coinfection with human immunodeficiency virus (HIV) which significantly increases the risk of developing TB.[2] Multidrug resistant (MDR) and extreme drug resistant TB, which are caused by poor case management, are a cause of serious concern throughout the world.[1]
Alarmed by the high prevalence, high mortality and morbidity due to TB globally World Health Organization (WHO) promoted a new effective TB control based on five essential elements called the Directly Observed Treatment Short Course (DOTS) strategy[3] India through Revised National TB Control Program of India adopted DOTS and achieved 70% case detection rate and cure rates (85%).[4]
Pulmonary TB (PTB) is the commonest and most infectious form of TB, but extra-PTB (EPTB) is becoming more rampant.[1,2] Female genital TB (FGTB) is an important form of EPTB, which is usually secondary to TB elsewhere in the body.[5] It causes significant morbidity, and short- and long-term sequelae, especially infertility for the affected women due to fibrosis and scarring occurring as a part of healing.[5]
EPIDEMIOLOGY
Genital tract TB has been reported in patients presenting with infertility, chronic pelvic pain, and menstrual irregularities, in autopsy series, and recently in laparoscopy series of infertility cases and pelvic pain.[5,6,7,8,9,10,11] It can even coexist with other diseases like endometriosis.[12] Incidence of genital TB in infertility cases varies greatly depending upon the geographical location being 1% in infertility clinics of United States,[10] 1.4% in Sweden,[11] 3.1% gynecological admissions in Malaysia,[12] 3.5 to 23% in Pakistan,[13,14] 0.8% (2% in tubal factor) in Italy,[15] 4.2% in infertility patients in Saudi Arabia,[16] 16.7% in Nigeria,[17] 6.15 to 21.1% in South Africa,[18,19] and 1 to 19% in various parts of India.[7,8,20,21]
In infertility, patients incidence of FGTB varies from 3 to 16% in India with higher incidence being from apex institutes like All India Institute of Medical Sciences, New Delhi where prevalence of FGTB in women of infertility was 26% and incidence of infertility in FGTB to be 42.5%, which may be due to referral of difficult and intractable cases to this apex hospital from all over India, especially from states like Bihar, Jharkhand, and Uttar Pradesh where prevalence of TB is very high.[5,8]
Incidence of FGTB is also very high in women enrolled for assisted reproduction technique (ART) being 24.5% overall, and in 48.5% with tubal factor infertility as reported by Singh et al.[22]
The prevalence of genital TB in infertility practices and infertility in various countries in FGTB, including in India by different authors, is shown in Tables 1 and 2.


FGTB occurs in younger age group in developing countries with range being 20–40 years, whereas in developed nations, it is usually diagnosed in premenopausal women over the age of 40 years.[5,6,7,8,9,10,11] It may be due to younger age at marriage and childbearing in developing nations as compared to developed countries.[5,11]
PATHOGENESIS
The genital organs involved in FGTB are fallopian tubes (90–100%), uterus (50–80%), ovaries (20–30%), cervix (5–15%), and vagina and vulva (1–2%).[4,7] The site of involvement in primary genital TB can be cervix, vagina, or vulva.[4,7] The spread of TB from lungs and other sites is usually by hematogenous or lymphatic route. Less commonly, direct contiguous spread from nearby abdominal organs like intestines or abdominal lymph nodes can cause genital TB. The fallopian tubes are involved in 90–100% cases with congestion, miliary tubercles, hydrosalpinx, pyosalpinx, and tubo-ovarian masses.[4,7]
Fallopian Tubes
Fallopian tubes are involved in almost all (>90%) women in genital TB, and the involvement is usually bilateral. Various types of TB salpingitis can be TB endosalpingitis, exosalpingitis, interstitial TB salpingitis and Salpingitis isthmic nodosa.[5,10,11,24]
In tuberculous endosalpingitis, the infection starts from endosalpinx and is usually through hematogenous route of spread. The fallopian tube is thickened, enlarged, and tortuous. Sometimes unilateral or bilateral pyosalpinx may be formed due to caseation in the tubal wall and the collection of the cheesy material in the lumen with blockade of both ends of fallopian tubes due to fibrosis.[5,11,24] Dense pelvic adhesions are often formed around the tubes though some women may have tubo-ovarian mass without adhesions.[5,11,24] Intestinal obstruction can occur due to adhesions. Endosalpinges may sometimes be hyperplastic or edematous and may be totally destroyed, or there may be fusion of papillae in the endosalpinx making women more susceptible to ectopic gestation and infertility.[5,11,24] Sometimes granulomatous lesion with chronic inflammatory infiltrate with or without caseation may be seen in the tube.[5,11,24]
In tuberculous exosalpingitis, disease spreads from intestines and starts in the muscularis mucosa of the tube. Initially, there is hyperemic of fallopian tubes, ovaries and peritoneum of the pouch of Douglas with flimsy adhesions, and miliary tubercles on their surface. Later there are beaded tubes with calcification and tubal blockade, tubo-ovarian masses due to perioophoritis, hydrosalpinx, pyosalpinx, or massive adhesion formation.[5,11,24] Various grades of adhesions are formed between tubes and adjacent pelvic organs. In more severe cases, there may be multiple adhesions in peritoneal cavity with obliterated pouch of Douglas (Frozen pelvis).[5,11,24] There occur perihepatic adhesions (Fitz–Hugh–Curtis syndrome) and hanging gall bladder sign in FGTB and abdominal pelvic TB.[25,26] Ascending colonic adhesions and peritoneal adhesions can also be seen. Abdomino-pelvic TB can also masquerade like ovarian cancer in some cases.[28]
In interstitial tuberculous salpingitis, interstitial part of the tube shows thickening of the tube with inflammation, whereas in salpingitis isthmica nodosa, there is nodular thickening of the tube due to proliferation of tubal epithelium within the hypertrophied muscle layer as diagnosed on hysterosalpingography as small diverticulum.[5,11,24]
Uterus
Endometrium is affected in about 70% cases of FGTB.
Initially, there is no macroscopic disease, but caseation and ulceration occur in advanced stages; distortion of the cavity occur with varying from slight distortion to complete obliteration due to adhesions.
Total destruction of the endometrium may Occur in Asherman’s syndrome leading on to secondary amenorrhea and infertility with poor prognosis for treatment.[5,11,29] Microscopically, TB granulomas with or without caseation, epithelioid cells, and Langhans cells may be observed, especially in the premenstrual phase and near the endometrial surface. However, typical granulomas may not always form due to repeated sheddings of endometrium at menstruation. It has been suggested that even in the absence of typical granulomas, endometrial TB may be diagnosed in the presence of a focal collection of lymphocytes with or without the presence of dilated glands and destruction of the epithelium.[5,11,24]
Ovaries
Ovarian involvement occurs in 10–15% cases. There may be tubercles on the ovaries, adhesions, caseation, and tubo-ovarian cyst or mass formation. Sometimes ovary may be completely destroyed by the disease. Ovarian function and reserve may also be affected in FGTB and abdomino-pelvic TB.[30,31]
Peritoneum
Pelvic and abdominal peritoneum may be involved in disseminated TB with tubercles all over the peritoneum, intestines, and omentum; it may cause ascites and abdominal mass masquerading as ovarian cancer. In such cases, ascitic fluid tapping for bio-chemical analysis and peritoneal biopsy may confirm the diagnosis of TB and thus, avoiding a needless laparotomy.
Cervix
The cervix may be involved in 5% cases of genital TB usually as a downward extension of endometrial TB but may rarely be a primary disease transmitted by the partner through infected semen. It may present as polypoidal growth or ulceration and may resemble cervical cancer necessitating biopsy for confirmation of diagnosis.[32] Microscopic examination will differentiate between the two conditions showing granulomatous inflammation in TB.[5,24,32]
Vagina and Vulva
Their involvement is rare (1–2%) and is usually secondary to the extension from endometrium or cervix, but may rarely be primary due to transmission from an infected partner with tubercular epididymitis. There may be a hypertrophic lesion or a nonhealing ulcer on the vulva or vagina simulating malignancy necessating biopsy and histopathological examination to confirm the diagnosis and to rule out malignancy and other differential diagnosis like syphilis, lymphogranuloma venereum, and others.[5]
Pathogenesis of Infertility in Genital Tuberculosis
Both primary and secondary infertility is quite common in FGTB (40–80% among FGTB cases). Pathogenesis of infertility in FGTB can be as follows:
-
Tubal factors causing infertility in FGTB
Blockage of fallopian tubes occurs commonly in FGTB due to their involvement.
Loss of tubal function due to ciliary damage in FGTB causing infertility and ectopic pregnancy.
Perisalpingitis causing adhesions and tubo-ovarian mass formation.
Tubercular hydrosalpinx with or without obstruction occurs in 46% cases of FGTB which can adversely impact fertilization and embryonic implantation.[33,34] In in vitro fertilization (IVF) treatment, women with tubercular hydrosalpinx, have very low pregnancy rate, which is worse with bilateral (12%) as compared to unilateral hydrosalpinx (24%). Clinical pregnancy rates can be increased with salpingectomy. As inflammatory reaction within the ovarian cortex provokes production of macrophage-mediated harmful cytokines and growth factors within the intrafollicular fluid adversely affecting the development of the oocyte.[33,34] However, routine pre-IVF salpingectomyin all women with ultrasonologically visible hydrosalpinx is not recommended but is done if aspirated hydrosalpingeal fluid can be tested for toxin by mouse-embryo assay.[33,34]
-
Ovarian function causing infertility in FGTB
Defective ovarian function occurs in FGTB due to the tubo-ovarian mass formation, adhesions, anovulation, and poor ovarian reserve causing infertility as follows:
Endocrine disruption can occur in FGTB.
In proven genital TB, chronic anovulation has been observed.
Mycobacterium tuberculosis has antigonadotropic effect: necessitating more ampoules of gonadotropins in IVF cycle.
Women with genital TB have higher Day 3 follicle-stimulating hormone (FSH) level and relatively lower peak E2 level, thus requiring higher number of gonadotropin ampoules than controls.[33]
Mycobacteria inhibit the basal production of progesterone and antagonize the stimulatory effect of human Chorionic Gonadotropin on corpus luteum, causing a luteal phase defect, implantation failure, lower pregnancy rates, and higher miscarriage rates.
In genital TB, quality of embryo tends to be poor due to “intrinsic oocyte factor” defect.[33] The harmful interleukins (ILs) induced by immune modulation or by the direct effect of toxins of mycobacteria adversely affect the oocyte development within the follicle.[33]
Uterine (endometrial) factors causing infertility
Endometrial damage occurs in TB as follows:
-
Effect of Genital TB on Endometrial Receptivity
FGTB adverse impacts the endometrial markers which are essential to make the endometrium receptive for embryonic implantation.[33]
-
Defective vascularization of the endometrium occur in FGTB.
Activation of antiphospholipid antibodies occurs in the endometrium in the FGTB with reduced subendometrial blood flow due to involvement of basal layer of endometrium causing defection endometrial vascularization.
Through immunomodulation with production of enzyme procoagulase causing vascular thrombus formation.
Endometrial atrophy and synechiae formation – Involvement of endometrium by caseous or fibrocaseous lesions of FGTB causes Asherman’s syndrome (uterine synechiae) which is common in endometrial TB.[29] We observed through hysteroscope various grades of intrauterine adhesions in FGTB as: Gr-I 20.8%, Gr-II 28.5%, Gr-III 28.5%, Gr-IV 17.5% with other findings of TB like tubercles, and shaggy cavity with caseation on hysteroscopy.[35] We observed increased difficulties and complications encountered during hysteroscopy in women with genital TB like inability to distend the cavity, excessive bleeding uterine perforation and flare-up of genital TB.[36] Hysterosalpingographic findings in our study were a normal uterine cavity in 57.1%, an irregular cavity in 18.5%, a shrunken cavity in 2.8% and an irregular filling defect in 18.5% and synechiae in 17.1% of women.[37]
Defective or failed implantation in FGTB.
It occurs in the following ways[33]:
There is release of harmful cytokines and growth factors (IL2, IL8, and TNFα) in the endometrium.
There is production of symmetric antibodies
There is production of natural killer cells
There is production of lymphocyte activated killer cells
-
There is T-helper-1 cell (Th-1) response with leads to implantation failure instead of T-helper-2 cell (Th-2) response needed for successful implantation of fertilized ovum.
Hence, FGTB shifts Th-2 response to Th-1 response in endometrium leading on to implantation failure. In fact, Dam et al.[38] from Kolkata observed latent FGTB to be an important cause of repeat IVF failure in their setting.
Diagnosis: Various Clinical Symptoms and Sings of Female genital tuberculosis Are Shown in Table 3[5,6,10,11,12]
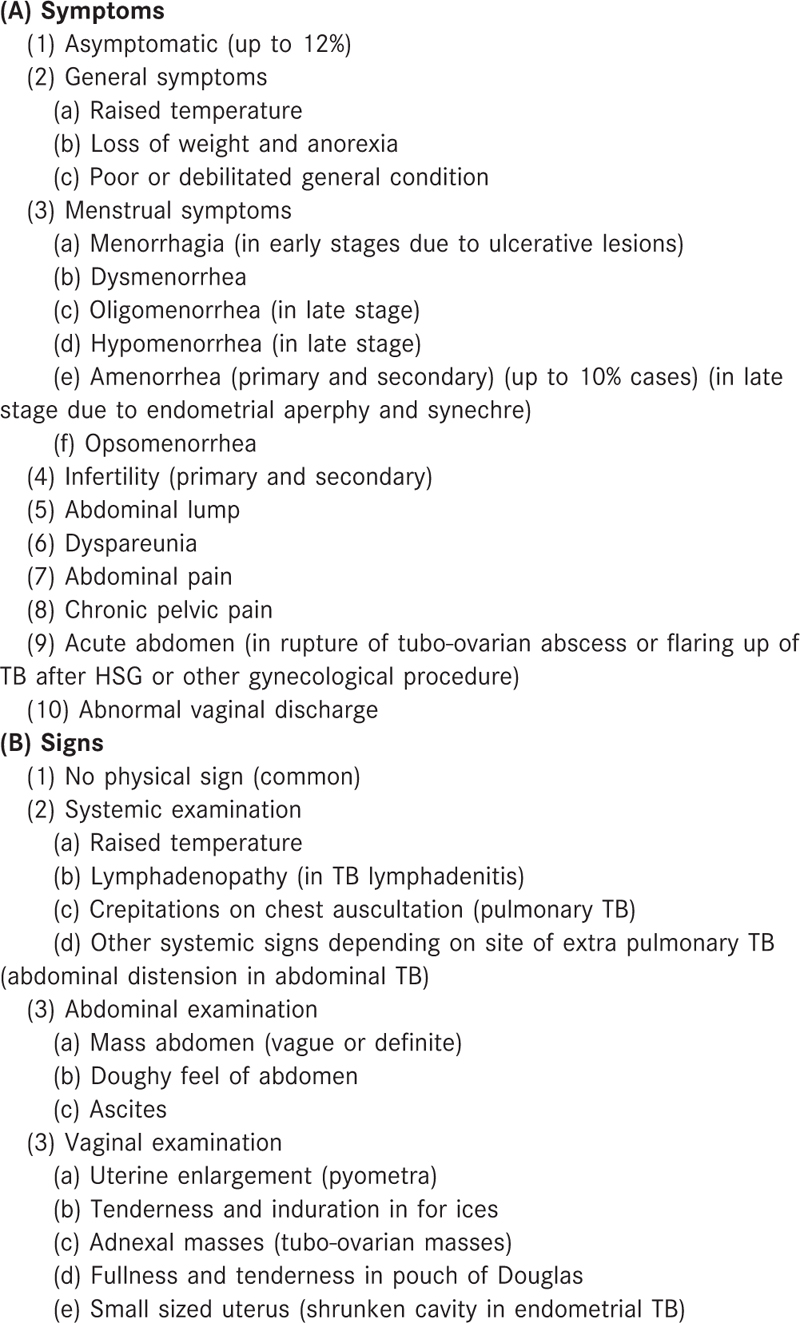
Early diagnosis of FGTB is essential for timely treatment and prevention of complication of FGTB especially fibrosis and infertility. A high index of suspicion is needed. Family or past history of TB goes in favor of FGTB. History of HIV positivity is also important. Detailed general physical examination for any lymphadenopathy, any evidence of TB at any other site in body (bones, joints, skin, etc.), chest examination (PTB), abdominal examination (abdominal TB), examination of external genitalia (vulvar or vaginal TB), speculum examination (cervical TB), and bimanual examination (endometrial or fallopian tube TB) helps in the diagnosis of genital TB.[5,11]
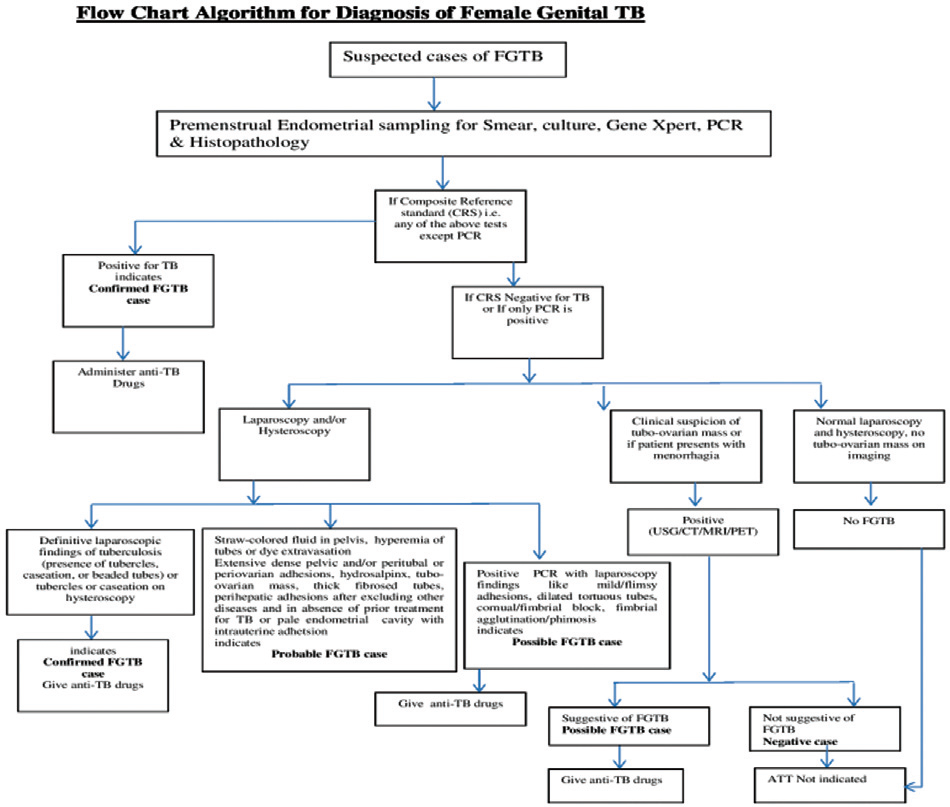
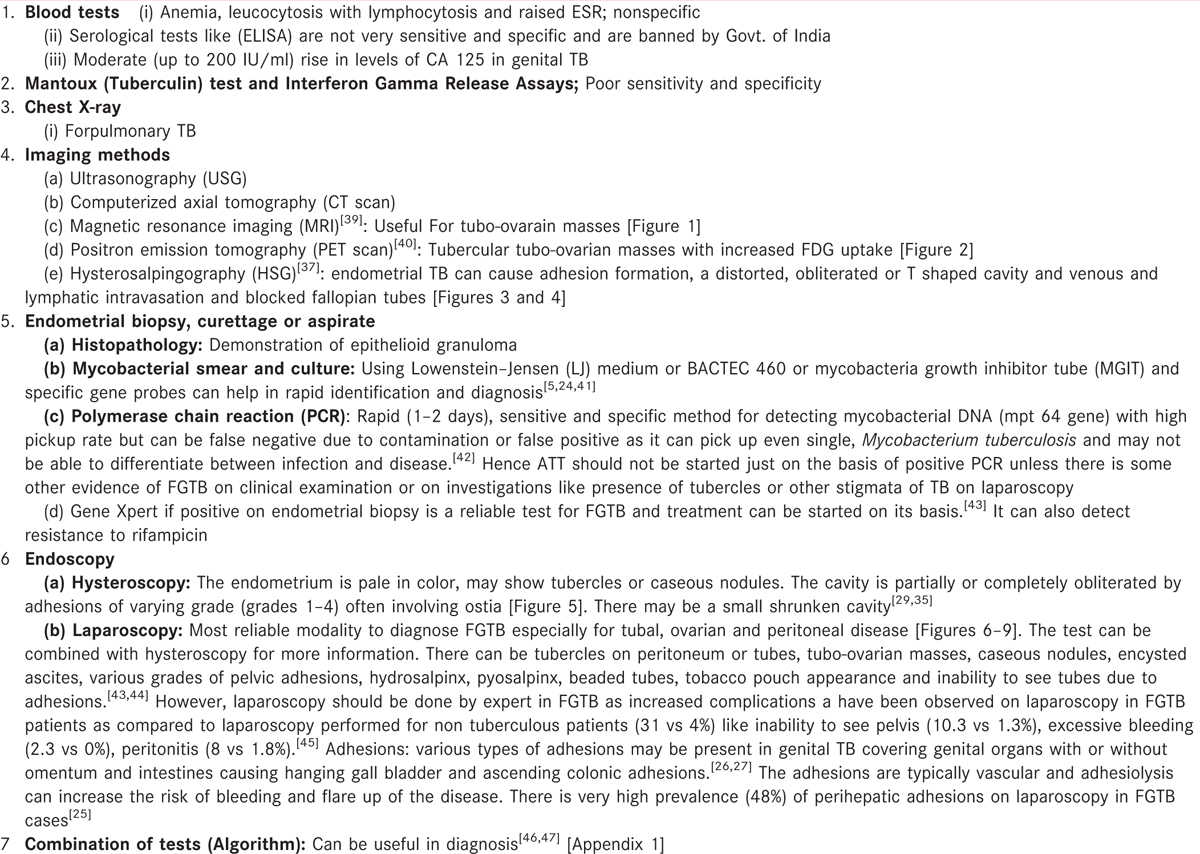
All tests are not required for every single case of genital TB. The tests will depend upon the site of TB and its clinical presentation and are shown in Table 4.[35,36] INDEX TB guidelines for extra-PTB, including FGTB, have been developed by Ministry of Health and family Welfare, Govt. of India and WHO and All India Institute of Medical Sciences in 2016 for guidance and management of FGTB.[47]
TREATMENT
Medical Treatment
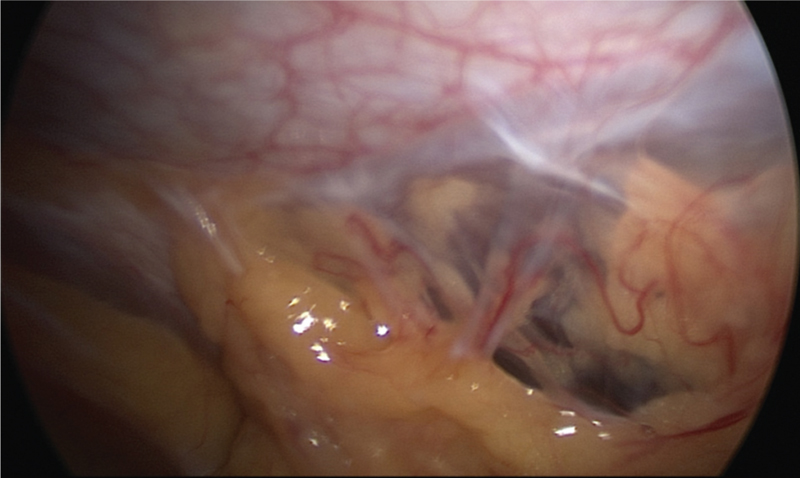
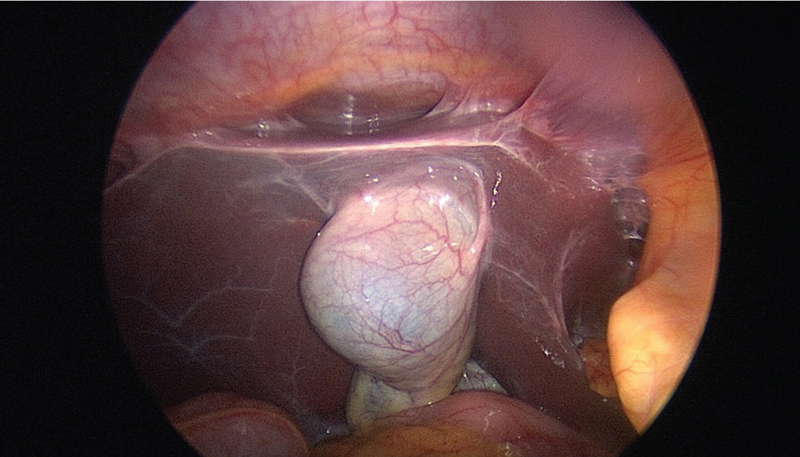
Treatment of latent genital TB detected only on positive polymerase chain reaction (PCR) is controversial due to high false positivity. Many assisted reproductive technology (ART) experts routinely treat positive PCR patients with better pregnancy outcome in those women treated with anti tubercular therapy (ATT) than without treatment. The logic of treating later TB is that in early stage, it can be treated without causing permanent damage to endometrium and other genital organs with much better outcome Jindal et al.[48] observed 30.8% pregnancy rate an TB PCR positive women with ATT, whereas Kulshrestha et al.[49] also obtained 31% pregnancy rate on ATT in TB PCR positive women. Latent genital TB has been found to be associated with repeated IVF failure in Indian clinical setting.[38] Even Indian on migration to Western countries, Indian women have poor prognosis with IVF as compared to Caucasian women despite similar embryo quality which could be due to latent FGTB in Indian women.[50] However, treating women with positive PCR is associated with risk of over treatment as many women without FGTB are then treated. Short course chemotherapy for 6–9 months has been found to be effective for medical treatment of FGTB[5,24] [Figures 1-9].
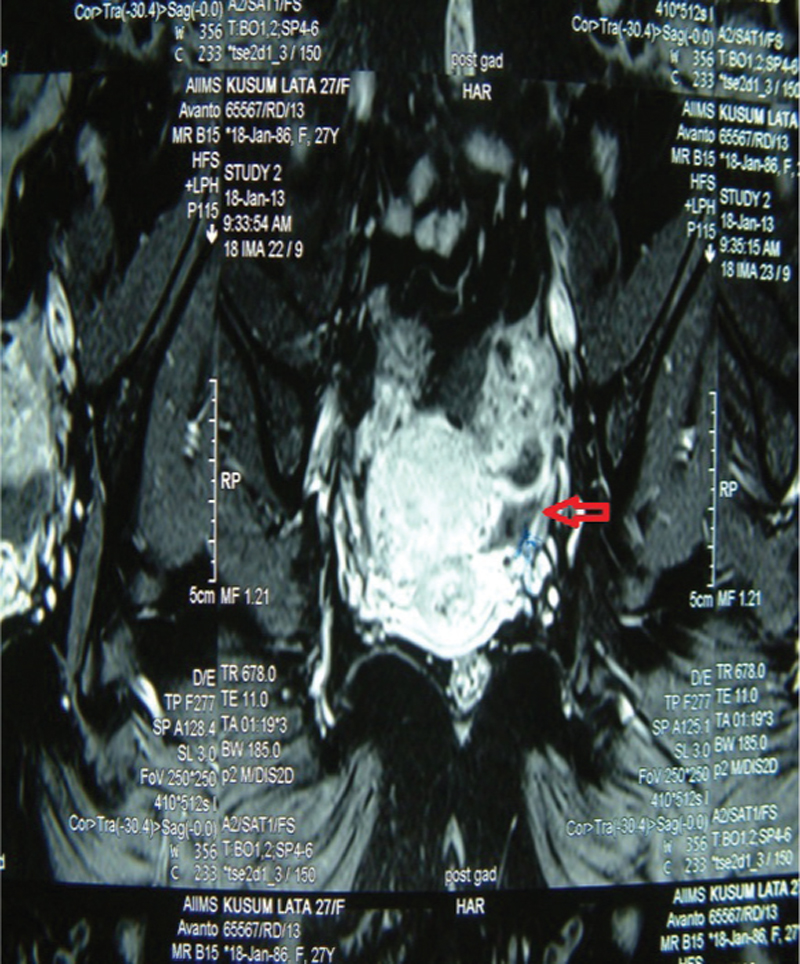
- MRI showing unilateral tubo-ovarian mass (arrow) in a case of FGTB
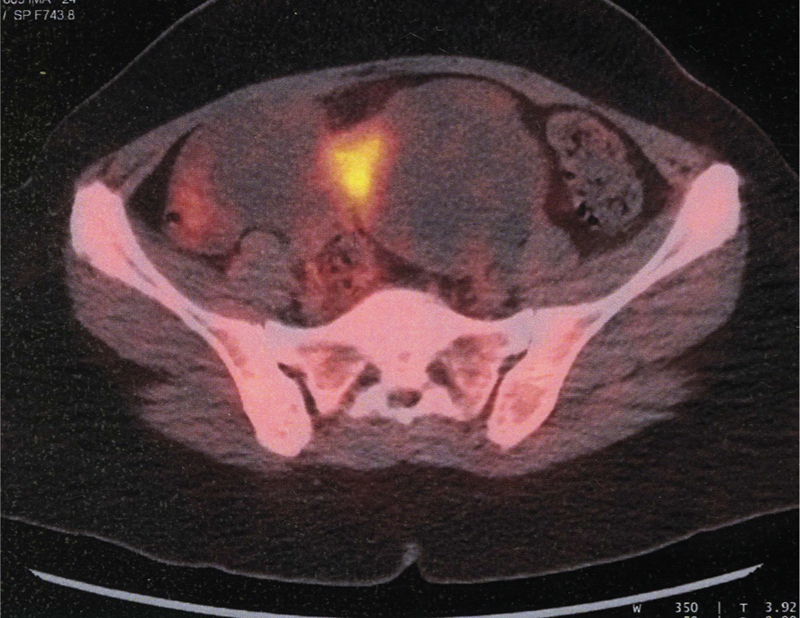
- FDG PET–CT showing unilateral tubo-ovarian mass (arrow) in a case of FGTB
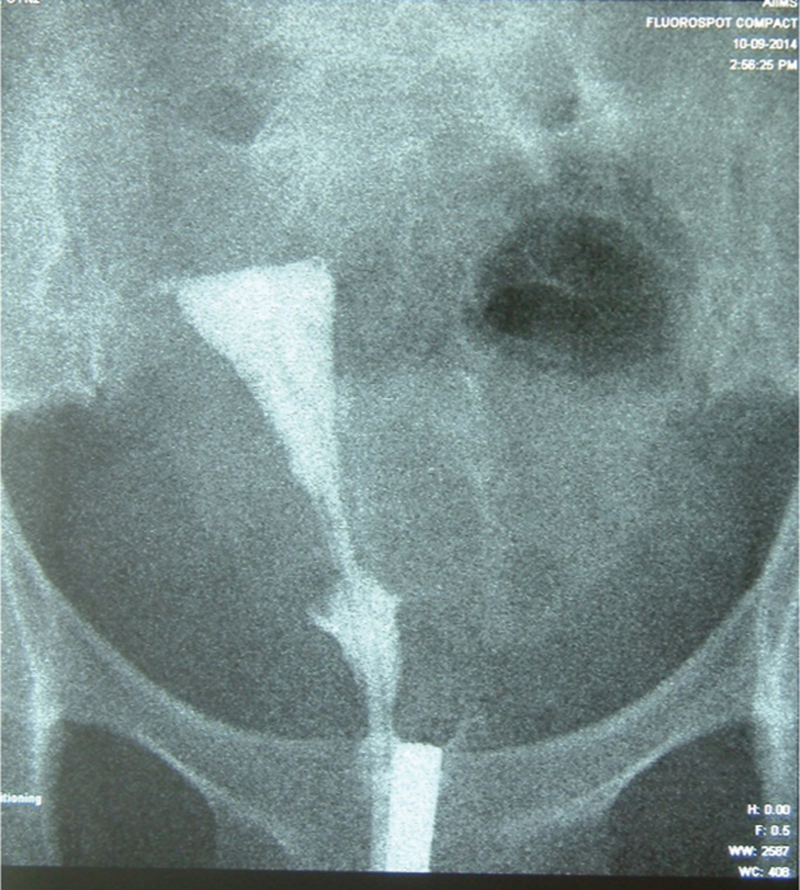
- Hysterosalpingography showing bilateral cornual block in a case of FGTB

- Hysterosalpingography showing bilateral tubes with a block rigid pipe stem appearance with venous intravasation on the left side in a case of FGTB
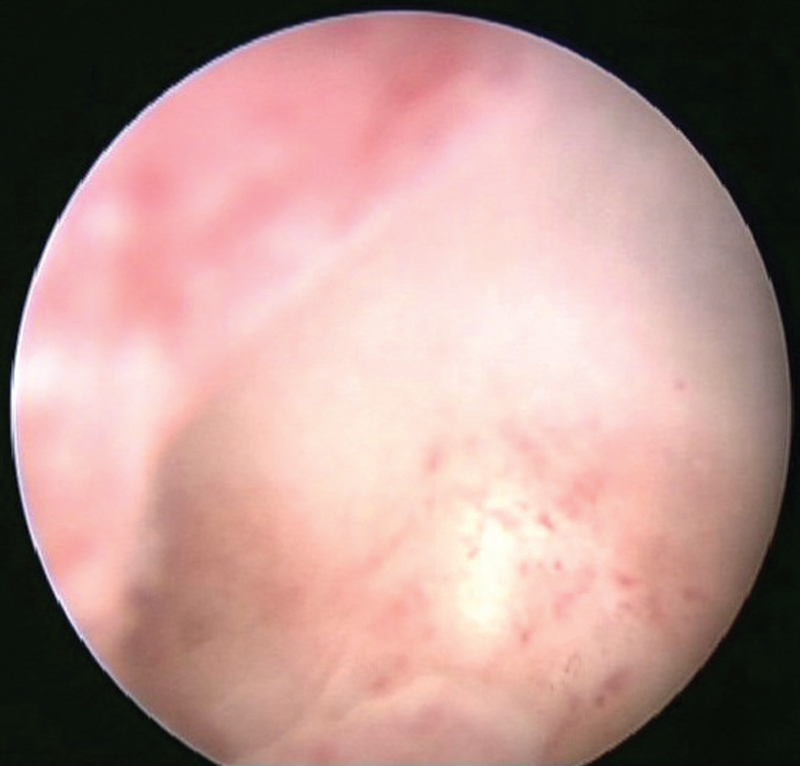
- Hysteroscopy showing pale endometrium and grade I adhesions in a case of FGTB
- Laparoscopy showing multiple abdominal and peritoneal adhesions in a case of FGTB
- Laparoscopy showing Grade II perihepatic adhesions (Fitz-Hugh–Curtis syndrome) and hanging gall bladder in a case of FGTB
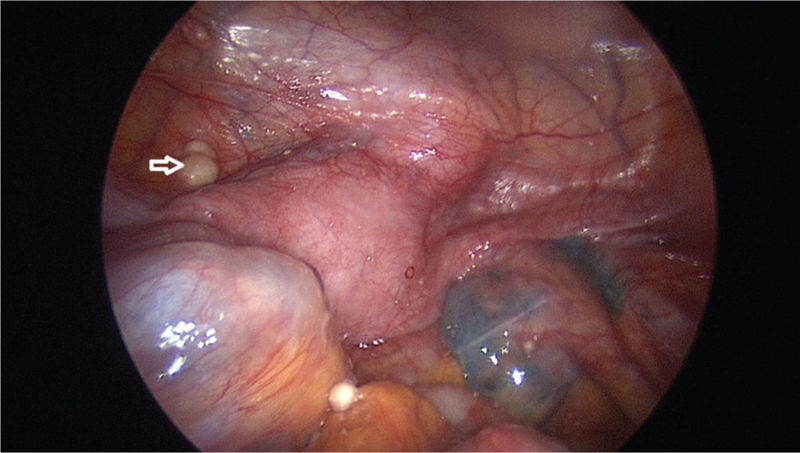
- Laparoscopy showing caseous nodules on peritoneum (arrow), hydrosalpinx in fallopian tubes and adhesions pouch of Douglas in a case of FGTB
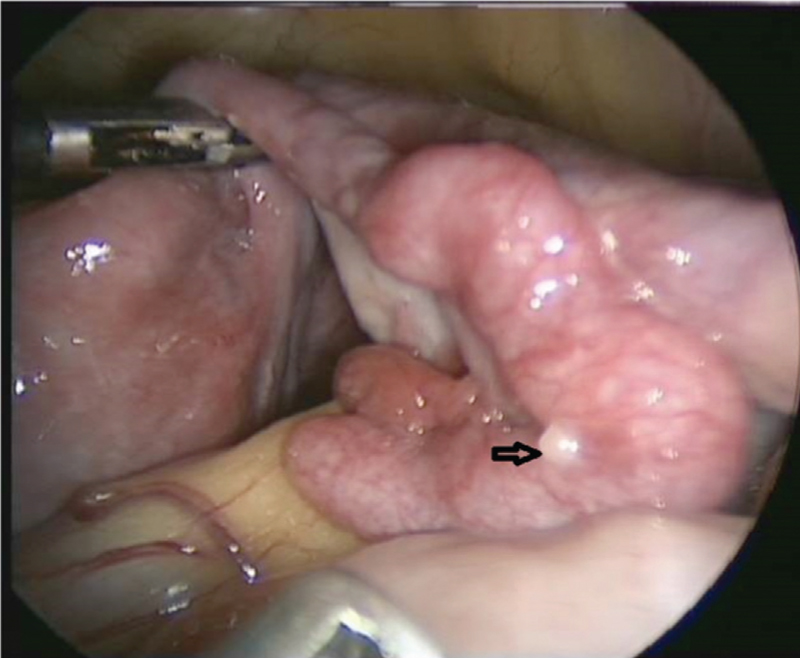
- Laparoscopy showing hyperemic and congested tubes with multiple tubercles (arrow)
In a randomized controlled trial, we observed 6 months antitubercular therapy with rifampicin, isoniazid, pyrazinamide, and ethambutol to be as effective as 9 months therapy confirming that 6 months therapy is adequate for FGTB.[51]
Directly Observed Treatment Short Course Strategy Treatment
DOTS is favored by WHO to prevent MDR and for better results. WHO in its recent guidelines has removed category III and recommend daily therapy of rifampicin (R), isoniazid (H), pyrazinamide (Z), and ethambutol (E) for 2 months followed by daily 4-month therapy of rifampicin (R) and isoniazid (H). Alternatively, 2 months intensive phase of RHZE can be daily followed by alternate day continuation phase (RH) of 4 months. Three weekly dosing throughout therapy (2RHZE 4HR) can be given as DOTS provided every dose is directly observed and the patient is not HIV positive or living in an HIV prevalent setting.[5,24,51]
The patient is first categorized to one of the treatment categories and is then given treatment as per guidelines for national programs by WHO [Table 5]. Genital TB is classified under category I being seriously ill extra pulmonary disease. To ensure quality-assured drugs in adequate doses a full 6-month course pack box is booked for an individual patient in the DOTS center with fixed drug combipack (FDC) of isoniazid, rifampicin, pyrazinamide, and ethambutol thrice a week for first 2 months (intensive phase) under direct observation followed by combination blister pack of isoniazid and rifampicin thrice a week for next 4 months (continuation phase).
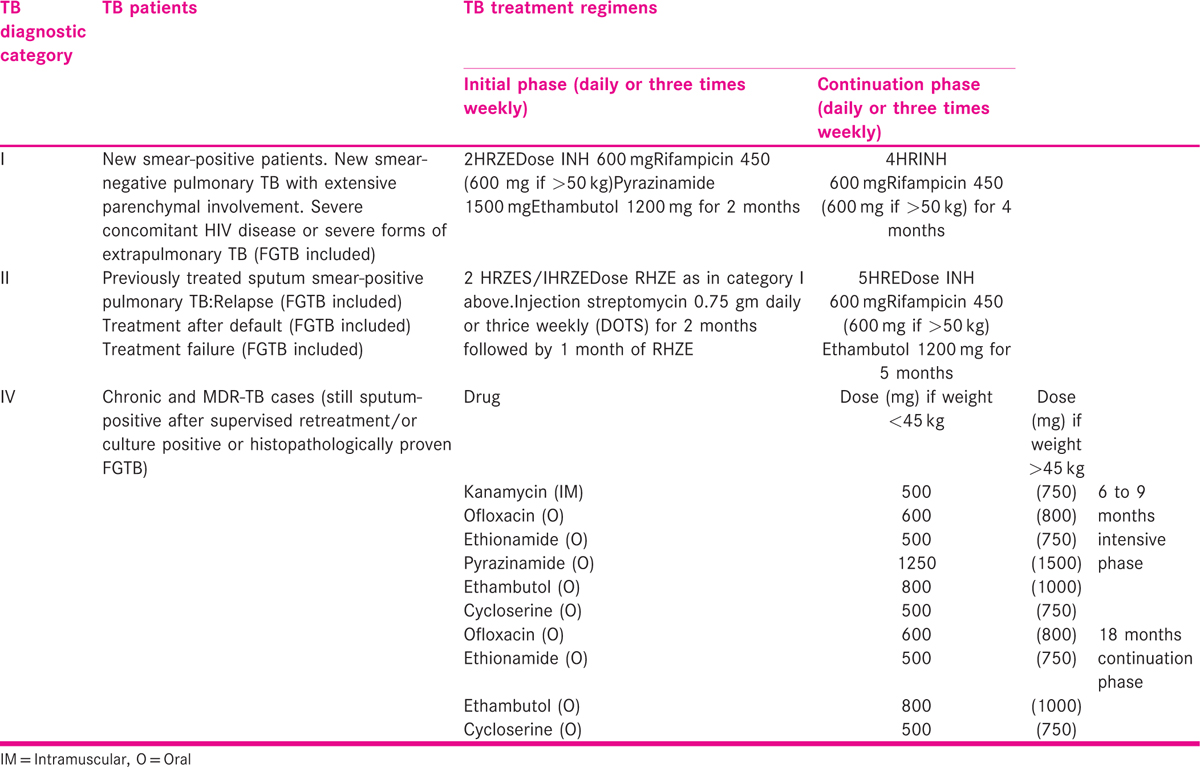
Sometimes, FGTB cases can have relapse or failure categorizing them into category II [Table 5], which includes 2-month intramuscular injections of streptomycin thrice weekly along with other four drugs (RHZE) of category I under direct supervision of DOTS centre health worker for first 2 months followed by four drugs (RHZE) thrice a week for another month (Intensive phase) followed by continuation phase with three drugs isoniazid (H), rifampicin (R), and ethambutol (E) thrice a week for further 5 months.
Non-DOTS treatment
Patients not opting for DOTS treatment must take daily therapy of RHZE for 2 months (intensive phase) followed by RH for 4 months (continuation phase). Convenient and economic combipacks are available in market.
Treatment of Chronic Cases, Drug Resistant, and Multidrug Resistant Female Genital Tuberculosis
Although rare, MDR FGTB is being observed in clinical practice. It is usually secondary for MDR TB in lungs or elsewhere but can be primary also if the initial infection occurs with MDR stains.[52] It is same as for pulmonary MDR with second-line drugs and is shown in Table 5 and is needed for long duration (18–24 months). Patients with HIV and TB should be treated with both antitubercular therapy and ATT in consultation with experts in the area.
MONITORING
The women should be counseled about the importance of taking ATT regularly and consumption of good and nutritious diet and should report in case of any side effects of the drugs. Liver function test are no longer done regularly unless there are symptoms of hepatic toxicity. Similarly, pyridoxine is not routinely prescribed with ATT unless there are symptoms of peripheral neuropathy with isoniazid. Rarely hepatitis can be caused by isoniazid, rifampicin, and pyrazinamide, optic neuritis by ethambutol and auditory, and vestibular toxicity by streptomycin, in which the opinion of an expert should be sought for restarting the ATT in a modified form.
Surgical Treatment
As general principle, surgery is avoided in FGTB as modern short course chemotherapy consisting of rifampicin and other drugs is highly effective for the treatment of FGTB. However, limited surgery like drainage from residual large pelvis or tubo-ovarian abscesses, pyosalpinx can be performed followed by ATT for better results. Besides, there are difficulties and much higher chances of complications during various surgeries like hysteroscopy, laparoscopy, and laparotomyin women with genital TB.[36,45,53] There is excessive hemorrhage and nonavailability of surgical planes at time of laparotomy with higher risks of injury to the bowel and other pelvic and abdominal organs.[53] In a case of abdomino-pelvic TB, bowel loops may be matted together with no plane between them, and uterus and adnexa may be buried underneath the plastic adhesions and bowel loops and is inapproachable. Even trying to perform a diagnostic laparoscopy or laparotomy in such cases can cause injury to bowel necessitating a very difficult laparotomy and resection of injured bowel.[45,53] It is better to take biopsies from the representative areas and close the abdomen without pelvic clearance in cases of laparotomy done for suspected pelvic tumors but found to be tubercular at laparotomy followed by full medical treatment.
Sometimes even after a full 6-month course of ATT, women with genital TB with infertility do not conceive when laparoscopy and hysteroscopy may be repeated to see any remaining disease which is then treated with category II drugs. It also useful to prognosticate and plan for further treatment. Outcome for fertility in FGTB is only good when ATT is started in early disease. However, cases of advanced TB with extensive adhesions in pelvis and uterus are usually not amenable to treatment with poor prognosis for fertility. Tuboplasty performed after ATT does not help much with chances of flare up of the disease and risk of ectopic pregnancy, should the women conceive.[54,55,56]
In Vitro Fertilization and Embryo Transfer in Female Genital Tuberculosis[57,58,59,60,61,62,63,64]
Most women with genital TB present with infertility and have poor prognosis for fertility in spite of ATT. The conception rate is low (19.2 %) with live birth rate being still low (7%).[21] In vitro fertilization with embryo transfer (IVF with ET) appears to be the only hope for some of these women whose endometrium is not damaged with pregnancy rate of 16.6 % per transfer.[57,58,59,60,61] Jindal et al.[48] observed favorable infertility outcomes following antitubercular treatment prescribed on sole basis of positive PCR, test for endometrial TB. Singh et al.[65] observed poor endometrial blood flow in women with FGTB undergoing IVF–ET. We also observed decreased blood flow to endometrium and ovaries in FGTB patients which got improved on repeat examination after ATT.[66,67]
Malhotra et al.[68] studied perifollicular Doppler blood flow before oocyte recovery in patients with or without genital TB. Although they observed a trend of poor ovarian blood flow in FGTB patients, there was no difference in other outcome variables like fertilization or cleavage rate in FGTB women undergoing IVF/ICSI in their center. IVF–ET has been found to be most successful out of all ART modalities in genital TB patients with 17.3 % conception rate in contrast to only 4.3 % with fertility enhancing surgery.[58] Latent genital TB has been found responsible for repeated IVF failure in young Indian patients presenting with unexplained infertility with apparently normal pelvis and nonendometrial tubal factors.[38] The pregnancy rates and take home baby rate could be improved by early detection when there is minimal damage and aggressive management of the disease. As already discussed in pathogenesis and pathology, women with FGTB have poor ovarian reserve with few quality embryos needing more gonadotropins, have poor endometrial receptivity or have endometrial synechiae. The result of IVF and ET are poorer than in other indications. The results of IVF–ET in FGTB by various authors are shown in Table 6 and pregnancy rate vary from 9.1 to 38.3% with many ending into abortion or ectopic pregnancy. Studies have shown poor result with IVF in FGTB due to the following reasons:
Most patient are poor responders.
Need high starting and maintenance dose of gonadotropins.
Endometrium invariably is poorly developed and even exogenous estrogen may not help.
Oocyte and embryo quality and pregnancy rate are poor.
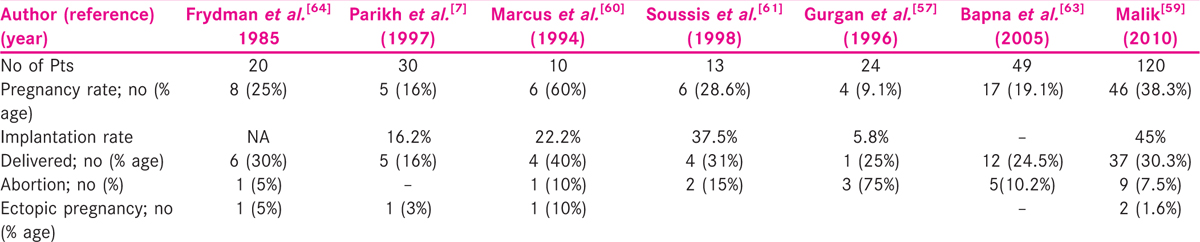
Malik[59] observed a pregnancy rate of 38.2% in 120 FGTB cases with IVF–ET which is comparable to other indications at her center. She attributed this to early diagnosis through molecular tests like PCR and aggressive management like that for active disease. ATT was given to the patients till the endometrial biopsy was negative and this varied from 6 to 18 months. IVF was done only after the biopsy was negative. Maximum number of pregnancies were achieved when treatment was given for 9 months (40%). No difference in pregnancy rate was noticed when patients were kept on or were taken off the ATT during the IVF cycle.
Hence, if after ATT, their tubes are still damaged, but their endometrium is receptive (no adhesions or mild adhesions which can be hysteroscopically resected), IVF–ET is recommended to these women.[59] However, if they have endometrial TB causing damage to the endometrium with shrunken small uterine cavity with Asherman’s syndrome, adoption or gestational surrogacy is advised to them.
GESTATIONAL SURROGACY IN GENITAL TB
It is advised in women with blockage fallopian tube or nonreceptive endometrium (Asherman’s syndrome).
In gestational surrogacy, another women’s uterus is used for implantation, whereas ovum belongs to this women and sperm belongs to her husband. She is, thus, the genetic mother of the fetus. The most important prerequisite for surrogacy in FGTB is a normal ovarian reserve with normal basal FSH (less than 10 IU/ml) level, ovarian volume (>3 ml), and basal antral follicular count of 4 or more.[69]
The indications of surrogacy in FGTB in India as advisable by Samanta et al. are as follows[69]:
Moderate-to-severe intrauterine adhesions not amenable to hysteroscopic adhesiolysis.
Atrophy of the basal layer of endometrium not responding to hormonal therapy.
Grossly reduced endometrial thickness (<7 mm) in spite of estrogen supplementation with high resistance subendometrial blood flow in the proliferative phase in repeated cycles.
Dense pelvic adhesions causing to repeated IVF failure.
Unexplained repeated IVF failure with endometrium showing persistence of TB granuloma or PCR positivity despite adequate antitubercular chemotherapy.
MDR genital TB
Surrogate host can be a family member or stranger but a friendship, must be established between host and the commissioning couple in surrogacy.
In their experience of surrogacy in FGTB at Institute of Reproductive Medicine in Kolkata on 14 women with uterine synechiae, poor endometrial development or repeated IVF failure, Samanta et al.[69] could achieve a viable delivery rate of 50%.
Adoption
If in spite of ATT, the fallopian tubes are blocked, endometrium is nonreceptive and even ovaries are nonfunctional, then adoption is advised to the couple.
New TB Research
There has been a renewed interest in research in TB globally with development of new drugs and vaccines. Newer diagnostic tests, including Gene Xpert, are being developed.[43,70] New drugs, effective against strains that are resistant to conventional drugs and requiring a shorter treatment regimen are being developed. There may be role of stem cell therapy in endometrial atrophy (Asherman’s syndrome) in FGTB to help regenerate the endometrium and tubal mucosa. IVF–ET if performed on time has good success rate. There is need to improve pregnancy outcome by IVF–ET in FGTB. Gestational surrogacy has a role in some women.
SUMMARY AND CONCLUSION
FGTB is in important cause of infertility being responsible for up to 16% cases of infertility in developing countries, while infertility is seen in up to 40–50% cases of genital TB.
FGTB can cause destruction of ovaries, tubo-ovarian masses, or poor ovarian reserve with poor quality of embryos and need of high dose of gonadotropins.
Endometrial TB cause poor endometrial receptivity, endometrial adhesions, and recurrent implantation failure.
Diagnosis is by good history taking, thorough clinical examination, and judicious use of investigations especially endometrial sampling for acid fast bacilli culture, PCR, and histopathological testing. Laparoscopy and hysteroscopy may be helpful in early diagnosis and to see the severity of disease for prognostication for fertility. Diagnostic algorithm (appendix) is very useful for making diagnosis of FGTB.
Medical treatment using DOTS strategy under direct observation and using quality-assured drugs in appropriate dosage and for adequate time is the mainstay of treatment.
Surgical treatment is rarely required and should only be done in exceptional circumstances and should be in the form of limited surgery like laparoscopy, hysteroscopy, and drainage of abscess, and so on, as surgery in genital and peritoneal TB can be difficult and hazardous.
Prognosis for fertility is poor. However, for tubal disease in absence of endometrial disease, ART especially IVF–ET may give good results if performed on time after giving full course of ATT and in fact may be the only hope for such women.
There is role of gestational surrogacy in women with Asherman’s syndrome due to endometrial TB with viable pregnancy rate of about 50%.
Stem cell therapy may play a role in regeneration of endometrium and tubal mucosa in FGTB in future.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
Author is thankful to Prof. Alka Kriplani, Professor and Head, Prof. Sunesh Kumar, Unit Head and Pawan for their help.
REFERENCES
- Global TB Report 2016. Geneva: World Health Organisation (WHO); 2016. WHO/HTM/TB 2016.
- Global Tuberculosis Control: Surveillance, Planning, Financing. In: WHO/HTM/TB 2006. Geneva: WHO; 2006. p. :362.
- [Google Scholar]
- WHO Report on the TB Epidemic. In: TB—A Global Emergency. WHO/TB/94-177. Geneva: WHO; 1994.
- [Google Scholar]
- Revised National Tuberculosis Control Program (RNTCP). Annual Status Report. In: Central TB Division, Directorate General of Health Services. Nirman Bhawan, New Delhi, India: Ministry of Health and Family Welfare; 2016. http://www.tbcindia.nic.in
- [Google Scholar]
- Tuberculosis and gynecological practice. In: Studd J, Tan SL, Chervenak FA, eds. Current Progress in Obstetrics and Gynecology (1st). Mumbai: Tree Life India; 2012. p. :304-27.
- [Google Scholar]
- Genital tuberculosis—a major pelvic factor causing infertility in Indian women. Fertil Steril. 1997;67:497-500.
- [Google Scholar]
- Genital tuberculosis in Indian infertility patients. Int J Gynaecol Obstet. 2007;97:135-8.
- [Google Scholar]
- Comparative study of laparoscopic abdominopelvic and fallopian tube findings before and after antitubercular therapy in female genital tuberculosis with infertility. J Minim Invasive Gynecol. 2016;23:215-22.
- [Google Scholar]
- Genital tuberculosis: an important cause of ectopic pregnancy in India. Indian J Tuberc. 2014;61:312-7.
- [Google Scholar]
- Incidence of genital tuberculosis in infertile women. J Pak Med Assoc. 1985;35:280-1.
- [Google Scholar]
- A histopathological study of endometrial tuberculosis in infertility. J Pak Med Assoc. 1992;42:269-70.
- [Google Scholar]
- Incidence of genital tuberculosis in infertile patients submitted to diagnostic laparoscopy: recent experience in an Italian University Hospital. Int J Fertil. 1991;36:104-7.
- [Google Scholar]
- The pattern of female genital tuberculosis in Riyadh, Saudi Arabia. Br J ObstetGynaecol. 1986;93:367-71.
- [Google Scholar]
- Genital tuberculosis in infertile women in northern Nigeria. West Afr J Med. 1993;12:211-2.
- [Google Scholar]
- Genital tuberculosis at Tygerberg Hospital—prevalence, clinical presentation and diagnosis. S Afr Med J. 1992;81:12-5.
- [Google Scholar]
- Tuberculosis of the female genital tract in patients attending an infertility clinic. S Afr Med J. 1990;77:562-4.
- [Google Scholar]
- Infertility and pregnancy outcome in female genital tuberculosis. Int J Gynaecol Obstet. 2002;76:159-63.
- [Google Scholar]
- Genital tuberculosis: a leading cause for infertility in women seeking assisted conception in North India. Arch Gynecol Obstet. 2008;278:325-7.
- [Google Scholar]
- Female genital tuberculosis. In: Sharma SK, Mohan A, eds. Tuberculosis (3rd). Delhi: Jaypee; 2016. p. :311-24.
- [Google Scholar]
- High prevalence of Fitz-Hugh-Curtis syndrome in genital tuberculosis. Int J Gynecol Obstet. 2007;99:62-3.
- [Google Scholar]
- Sharma’s hanging gall bladder sign: a new sign for abdominopelvic tuberculosis: an observational study. J IVF Lite. 2015;2:94-8.
- [Google Scholar]
- Sharma’s ascending colonic adhesion: a new sign in abdominopelvic tuberculosis with infertility. J IVF Lite. 2016;3:18-22.
- [Google Scholar]
- Abdomino-peritoneal tuberculosis masquerading as ovarian cancer: a retrospective study of 26 cases. Arch Gynecol Obstet. 2010;282:643-8.
- [Google Scholar]
- Genital tuberculosis: an important cause of Asherman’s syndrome in India. Arch Obstet Gynecol. 2008;277:37-41.
- [Google Scholar]
- The effect of tuberculosis on ovarian reserve among women undergoing IVF in India. Int J Gynaecol Obstet. 2012;117:40-4.
- [Google Scholar]
- Effect of antitubercular treatment on ovarian function in female genital tuberculosis with infertility. J Hum Reprod Sci. 2016;9:145-50.
- [Google Scholar]
- Cervical tuberculosis masquerading as cervical carcinoma: a rare case. J Obstet Gynaecol Ind. 2001;51:184-5.
- [Google Scholar]
- Genital tuberculosis-ovarian function and endometrial receptivity. In: Mukherjee GG, Tripathy SN, Tripathy SN, eds. Genital Tuberculosis (1st). New Delhi: Jaypee Brothers Medical Publishers (P) Ltd; 2010. p. :27-42.
- [Google Scholar]
- The significance of cytokines, chemical composition, and murine embryo development in hydrosalpinx fluid for predicting the IVF outcome in women with hydrosalpinx. Hum Reprod. 2002;17:128-33.
- [Google Scholar]
- Hysteroscopic findings in women with primary and secondary infertility due to genital tuberculosis. Int J Gynecol Obstet. 2009;104:49-52.
- [Google Scholar]
- Increased difficulties and complications encountered during hysteroscopy in women with genital tuberculosis. J Minim Invasive Gynecol. 2011;18:660-5.
- [Google Scholar]
- Hysterosalpingographic findings in infertile women with genital tuberculosis. Int J Gynecol Obstet. 2008;101:150-5.
- [Google Scholar]
- Role of latent genital tuberculosis in repeated IVF failure in Indian clinical settings. Gynecol Obstet Invest. 2006;61:223-7.
- [Google Scholar]
- Magnetic resonance imaging findings among women with tubercular tubo-ovarian masses. Int J Gynecol Obstet. 2011;113:76-80.
- [Google Scholar]
- Comparison of PET/CT with other imaging modalities in women with genital tuberculosis. Int J Gynaecol Obstet. 2012;118:123-8.
- [Google Scholar]
- Improved diagnostic value of PCR in diagnosis of female genital tuberculosis leading to infertility. J Med Microbiol. 2005;54:927-31.
- [Google Scholar]
- Role of Gene Xpert in diagnosis of female genital tuberculosis: a preliminary report. Eur J Obstet Gynecol Reprod Biol. 2016;207:237-8.
- [Google Scholar]
- Laparoscopic finding in female genital tuberculosis. Arch Gynecol Obstet. 2008;278:359-64.
- [Google Scholar]
- Increased complication rates associated with laparoscopic surgery among patients with genital tuberculosis. Int J Gynecol Obstet. 2010;109:242-4.
- [Google Scholar]
- An algorithmic approach to female genital tuberculosis causing infertility. Int J Tuberc Lung Dis. 2006;10:1045-50.
- [Google Scholar]
- Govt. of India and World Health Organization. INDEX TB Guidelines for diagnosis and management of extra-pulmonary tuberculosis. CEPTB in India 2016 March http://www.tbcindia.nic.in/showfile.php.led=3245
- [Google Scholar]
- Favorable infertility outcomes following anti-tubercular treatment prescribed on the sole basis of a positive polymerase chain reaction test for endometrial tuberculosis. Hum Reprod. 2012;27:1368-74.
- [Google Scholar]
- Genital tuberculosis among infertile women and fertility outcome after antitubecular therapy. Int J Gynecol Obstet. 2011;113:229-34.
- [Google Scholar]
- Poorprognosis with in vitro fertilization in Indian women compared to Caucasian women despite similar embryo quality. PLoS One. 2009;4:e7599.
- [Google Scholar]
- Six months versus nine months anti-tuberculous therapy for female genital tuberculosis: a randomized controlled trial. Eur J Obstet Gynecol Reprod Biol. 2016;203:264-73.
- [Google Scholar]
- Multi drug resistant female genital tuberculosis: a preliminary report. Eur J Obstet Gynecol Reprod Biol. 2016;210:108-15.
- [Google Scholar]
- Surgical complications during laparotomy in patients with abdominopelvic tuberculosis. Int J Gynecol Obstet. 2010;110:157-8.
- [Google Scholar]
- Postoperative flare-up of genital tuberculosis: a clinical reality. Int J Tuberc Lung Dis. 2008;12:981-3.
- [Google Scholar]
- Genital tuberculosis: an important cause of ectopic pregnancy in India. Indian J Tuberc. 2014;61:312-7.
- [Google Scholar]
- Genital tuberculosis in adolescent girls from low socioeconomic status with acute ectopic pregnancy presenting at a tertiary care hospital in urban Northern India: are we missing an opportunity to treat? Arch Gynecol Obstet. 2012;286:1477-82.
- [Google Scholar]
- Results of in vitro fertilization and embryo transfer in women with infertility due to genital tuberculosis. Fertil Steril. 1996;65:367-70.
- [Google Scholar]
- P-371. The place for IVF in genital tuberculosis. Hum Reprot. 2003;18(Suppl 1):XVIII. 126
- [Google Scholar]
- IVF and tuberculosis. In: Mukherjee GG, Tripathy SN, Tripathy SN, eds. Gential Tuberculosis (1st). Delhi: Jaypee Brothers Medical Publishers (P) Ltd.; 2010. p. :135-40.
- [Google Scholar]
- Tuberculosis infertility and in vitro fertilization. Am J Obstet Gynecol. 1994;171:1593-96.
- [Google Scholar]
- In vitro fertilization treatment in genital tuberculosis. J Assist Reprod Genet. 1998;15:378-80.
- [Google Scholar]
- Tuberculosis. In: Manula of Obstetrics and Gynaecologist (Ist). New Delhi: Jaypee The Health Sciences Publisher; 2015.
- [Google Scholar]
- Genital tuberculosis and its consequences on subsequent fertility. J Obstet Gynaecol Ind. 2005;55:534-7.
- [Google Scholar]
- In vitro fertilization in tuberculous infertility. J In Vitro Fert Embryo Transf. 1985;2:184-9.
- [Google Scholar]
- Comparative analysis of endometrial blood flow on the day of hCG by 2D Doppler in two groups of women with or without genital tuberculosis undergoing IVF-ET in a developing country. Arch Gynecol Obstet. 2011;283:115-20.
- [Google Scholar]
- Effect of antitubercular therapy on endometrial function in infertile women with female genital tuberculosis. Infect Disord Drug Targets. 2016;16:101-8.
- [Google Scholar]
- Effect of antitubercular treatment on ovarian function in female genital tuberculosis with infertility. J Hum Reprod Sci. 2016;9:145-50.
- [Google Scholar]
- Role of perifollicular Doppler blood flow in predicting cycle response in infertile women with genital tuberculosis undergoing in vitro fertilization/intracytoplasmic sperm injection. J Hum Reprod Sci. 2014;7:19-24.
- [Google Scholar]
- Gestational surrogacy in gential tuberculosis. In: Mukherjee GG, Tripathy SN, Tripathy SN, eds. Gential Tuberculosis (1st). Delhi: Jaypee Brothers Medical Publishers (P) Ltd.; 2010. p. :141-54.
- [Google Scholar]
- Evaluating PCR, culture & histopathology in the diagnosis of female genital tuberculosis. Indian J Med Res. 2011;134:40-6.
- [Google Scholar]
APPENDIX 1