

Translate this page into:
Association of body mass index (BMI) and sub-fertility among young women in Karachi, Pakistan
Address for correspondence: Mubashir Zafar, Department of Public Health, College of Public Health, Imamm Abdul Rahman Bin Faisal University, Dammam, KSA. E-mail: mzzahmed@iau.edu.sa
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objective:
The aim of the study is to determine the association of body mass index (BMI) with sub-fertility among young women in Karachi Pakistan.
Methods:
It is a case control study in which 284 participants were selected through simple random sampling technique and 142 divided into cases and control group. Cases were nulliparous women who were not able to conceive after 24 months of unprotected intercourse and controls were primigravida women. Validated questionnaire was given to patients, height and weight was measured and BMI was calculated. Odds ratio (OR) was calculated with logistic regression.
Results:
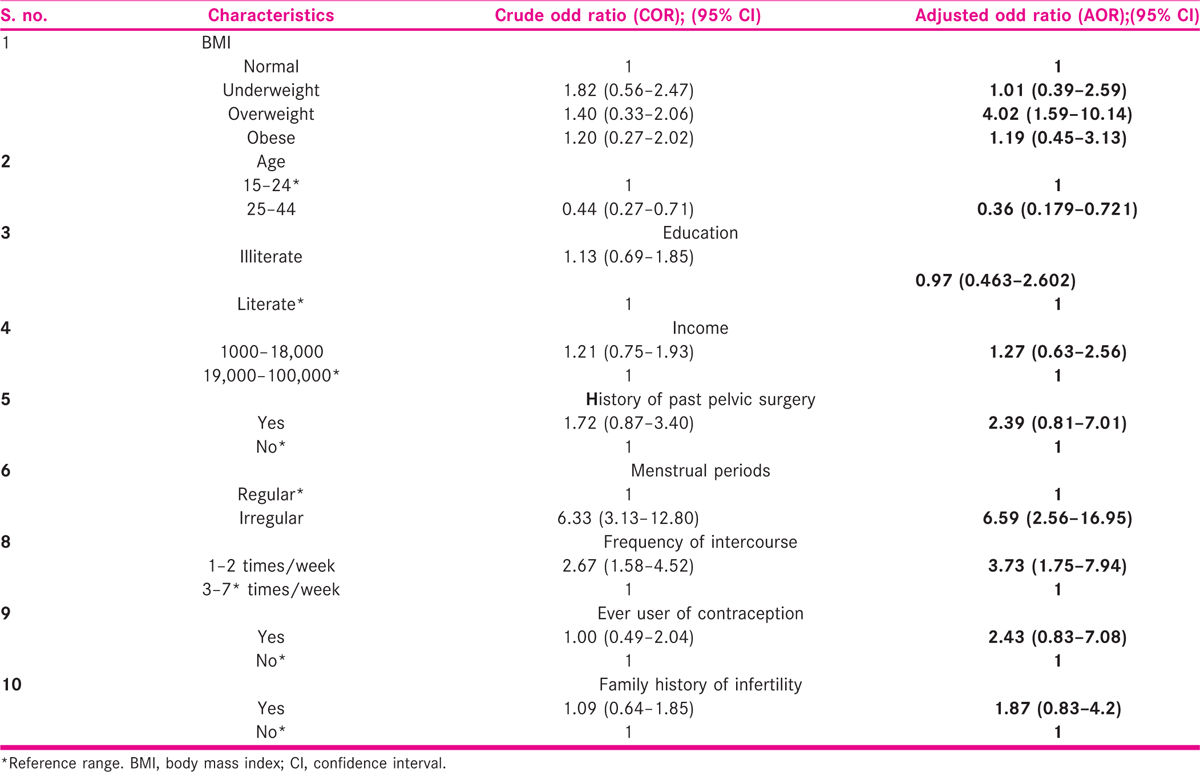
Mean age of the study participants were (25.3 years standard deviation ± 2.5). After adjustment of the covariates, women with high BMI (BMI 30 and above) were more than four times {OR 4.20 (95% confidence interval, CI, 1.59–10.14)} and women with BMI 25 to 29.9 were more than one times sub-fertile {OR 1.19 (CI 0.45–3.13)} compared to normal (BMI 20.0–22.4). The women with less frequency of intercourse (1–2 times/week) were more than three times {OR 3.73 (CI 1.75–7.94)} were sub-fertile.
Conclusion:
There is need for inventions to control BMI which increase fertility level among women. Nutritional modification requires to counter infertility because obese women require higher doses of medication and produce fewer follicles.
Keywords
BMI
body
pregnancy
primigravida
sub-fertility
weight
women

INTRODUCTION
Sub-fertility is a condition of inability of a sexually active couple to conceive for 1 year of sexual relationship.[1] Sub-fertility is a global issue and its prevalence worldwide is around 10% to 15%.[1] Many factors contribute to sub-fertility such as women’s age (>35 years), depression, stress, exposure to radiation, high temperature and pesticides, smoking, alcohol consumption, sexually transmitted diseases, underweight and overweight.[2]
The most common indicator for weight of a body is body mass index (BMI); it is calculated by weight in kilogram divided by height in metre square.[1] Low and high BMI causes the reproductive health dysfunction such as sub-fertility, infertility and dysfunction of ovulatory cycle.[2] Obesity is common among women which causes infertility due to impairment in ovulation and insulin resistance; these causes also lead to decrease in chance of becoming pregnant of women with normal cycles.[2,3] Different studies showed that young obese women who have a desire to conceive can opt for bariatric surgery that can solve the issue.[3,4,5]
Excess body weight will be affected female hormone levels.[6,7] A considerably reduced hormone level has been diagnosed among women whose BMI were high (BMI > 25) compared with normal BMI women.[8,9] Now several researches have been focused on lifestyles risk factors which effects infertility, specifically on alcohol, caffeine, tobacco, junk food and occupational exposures. Obesity has public health problem in affluent societies and consistent evidence has presented that menstrual disorder is associated with obesity. A very few studies have investigated the association of obesity with sub-fertility.[9,10]
Although Pakistan is ranked sixth among the most populous countries of the world and has a population growth rate of around 2%, sub-fertility rate in Pakistan is about 21.9% (3.5% primary and 18.5% secondary)[11,12]; it is more common among female because obesity in them is approximately 44% and in male is around 22%.[11]
In Pakistan, there is prevalence of sub-fertility among female; high BMI is one of the major factor which contributes to infertility and is increasing in an abnormal pace.[11] There is a need of such type of study that determines the association between sub-fertility and BMI which helps the policymaker in making their policies regarding sub-fertility management and educate the women to improve their lifestyle behaviour which leads to reduce the body weight. The aim of this study is to determine the association between sub-fertility with high and low BMI attending infertility clinic compared to another group of primigravida attending antenatal care.
METHODOLOGY
Operational definition
Sub-fertility is defined as the inability to conceive within first 2 years of marriage.
Fertility refers to spontaneous conception within 2 years of marriage.
BMI refers to the body mass index which is calculated by dividing weight in kilograms by height in metre square and is classified as underweight (<18), normal (18–24.9), overweight (25–29.9) and obesity (>30) in person.
Study area, study participants and study design
The study was carried out in Public Sector Hospital in the Department of Obstetrics and Gynaecology. This hospital is a tertiary care setup and busiest hospitals in the city which has 1000 beds and average outpatient department (OPD) around 10,000 patients per day. The study comprised females in their reproductive ages, that is from 18 to 35 years. The participants were selected from patients’ turnover in OPDs. Design of study was case and control. Control group consisted of 142 of primigravida. Case group consisted of 142 of primary sub-fertile females.
Sampling technique and sample size
Non-probability convenient sampling was used to select the study participants. Sample size of 284 was calculated by formula using proportion of sub-fertility level among obese individuals of the previous study.[13] It was estimated by using proportion of sub-fertility as 40% at confidence level 95%, power 80% and bound of error 3%.

For 80% power, Z = 0.84.
For 0.05 significance level, Z = 1.96.
r = 1 (equal number of cases and controls).
The proportion exposed in the control group is 20%.
To get proportion of cases exposed.
Inclusion and exclusion criteria
Fertile group (control)
Fertile group (controls) was selected as age between 18 and 35 years and women who were primigravida. Those women were excluded who had co-morbidities like diabetes, hypertension, asthma, bleeding disorder and ischaemic heart disease. Participants were treated for sub-fertility or opted for assisted conception. Any multi-gravid women were also excluded.
Sub-fertile group (case)
Sub-fertile group (cases) was selected as women who were unable to conceive after 2 years of sexual relationship and of age between 18 and 35 years. Those women were excluded who conceived previously but currently were unable to do so. Women with co-morbidities like diabetes, hypertension, asthma, bleeding disorder and ischaemic heart disease were also excluded. Any multi-gravid women, any secondary sub-fertile disease and second marriage of either partner were also excluded.
Study variables
Independent variable
This variable includes age, years of marriage, occupation, income, ethnicity, education, birth place, blood group, height, weight, exercise, vaccination, allergy, medication, previous surgery, screening, transfusion history, dietary habits, family history of sub-fertility and obesity, menstrual history, contraceptive and smoking.
Dependent variable
Sub-fertility is the dependent variable.
Data collection tool
Validated questionnaire was used which is divided into six sections. These questions were validated internally and externally. Before filling the questionnaire, each participant was asked for informed/signed consent individually. The section of questionnaire is as follows:
Participant’s socio-demographic status (age, years of marriage, occupation, income, ethnicity and education)
Medical history (height, weight, exercise, vaccination, allergy, medication, surgery, transfusion and radiation exposure)
Dietary history (eating habits, addiction and smoking)
Family history (history of obesity and infertility)
Reproductive history (menstruation and contraception)
Data collection procedure
Before the data collection, the administration of the hospital granted the permission and after getting the consent from patient, interview was conducted in the OPD. An average of 15 minutes was given for each interview and the body weight and height of the participants were measured.
Data management and analysis
After the data collection, it was coded using Excel sheet and then data entered in Epi Data software version 1.3; it was double entered because missing values were cleaned and error rate was determined accordingly. Data was analysed in SPSS, version 23.0 (SPSS Inc., Chicago, IL, USA) for statistical analysis. Mean and standard deviation were calculated for quantitative variables of socio-demographic characteristics. Chi-square test was applied for determining the difference of cases and control. For determination of association of sub-fertility and BMI, regression analysis was used.
Ethical approval
The study protocol was approved by the Ethical Committee of the Department. Permission was taken from respective departments and consent form signed from each participant before conducting an interview. Participation was voluntary and were free to withdraw at any time without any explanations. The confidentiality and privacy of the participants was maintained and there was no financial benefit to either the patient or the researcher.
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
RESULTS
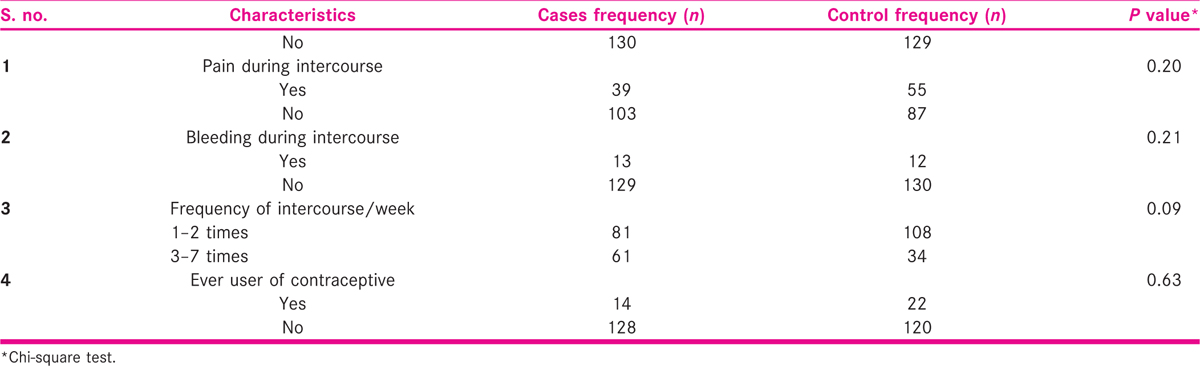
In Table 1, basic characteristic of case and control are given. Only education level and BMI were statistically difference between cases and control in basic characteristics.

There are only ages of menarche, regularity of menstrual cycle and excess facial hair which were statistical different among cases and control group regarding reproductive history [Table 2].
Those women whose BMI more than 30 (overweight) were more than four times {odds ratio, OR, 4.02; confidence interval, CI (1.59–10.14), menstrual period was irregular six times {OR 6.59; CI (2.56–16.95)} and frequency of intercourse one to two times a week had three times {OR 3.73; CI (1.75–7.94)} were associated with sub-fertility [Table 3].
DISCUSSION
Study result found four-fold increase risk of sub-fertility among overweight women compared to women of normal weight. These results show the association of BMI and sub-fertility and this is the first report in Pakistan which validates the association of BMI and sub-fertility.
Overweight related to biologic changes in the human body reduces the fertility. Different study results show reductions in sub-fertility with obesity.[14,15,16,17,18,19,20] A study of young women revealed sub-fertility among women with high BMI.[16] Another study report that those have overweight and obese had reduced conception ability.[21]
Women’s obesity studied[22,23] regarding infertility data shows that socioeconomic status is a key factor that affects person’s reproductive life (CI 0.632–2.565; OR 1.273); low socioeconomic class have 1.273 times more chances of developing infertility. A similar study result shows that primary infertility is 7.2% higher in lower socioeconomic status than higher socioeconomic status.[24]
Our results also pointed that infertility was associated with ill-literacy which is 1.13 times more than literate. A study was done to reveal that young educated people who were aware of risk factor of infertility had lesser chances of developing infertility.[25]
The association was more prominent in women who had family history of infertility; this result was validated by other study.[26] The study also revealed that irregular menstrual cycle is also a common factor for sub-fertility and this result is also validated by other study.[27]Smoking is also a common risk factor for sub-fertility, but the result is not significant because in our society tobacco chewing is common in both males and females. The result that smoking affects sub-fertility is also validated by other study.[28]
The marriage factors such as frequency of intercourse effects the conception of women and this study strongly associated with less frequency were contributed for sub-fertility and this is same result for other study conducted previously.[29]
Previous studies regarding BMI and infertility shows that increasing age was associated with more difficulty in attaining pregnancy.[30,31,32,33,34,35] This study shows that there is no difference regarding conception between low age and high age because of study participants which included only 35 years of women but other studies confirmed the difference between high and low age conception.
Limitation of this study is the women pregnancy status. The most crucial time was before pregnancy, when the couple first tried to make the women pregnant. Several studies would have an advantage from collection of data of BMI before the start of pregnancy.
The limitation of this study was that the study could not be conducted on more extensive grounds due to the lack of time and resources. Some of the anthropometric measurements taken into the data were measured at the time of data collection, whereas some were totally self-reported by the participants. However, maximum effort was done to obtain the optimum result possible within the parameters.
CONCLUSION
The study results confirm the association of BMI and sub-fertility as BMI four times increases the chance of sub-fertility. There is need for health education programme in society to build awareness specifically in women to consume health diet and promote physical activity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
The author extends his sincere appreciation to the Department of Public Health, Imam Abdulrahman Bin Faisal University, and the Public Sector Hospital in Karachi for provision of the necessary support that enabled him to fulfil this study.
REFERENCES
- Effects of obesity on women’s reproduction and complications during pregnancy. Obes Rev. 2004;5:137-43.
- [Google Scholar]
- Socioeconomic variations in female fertility impairment: a study in a cohort of Portuguese mothers. BMJ Open. 2014;4:39-85.
- [Google Scholar]
- Reproductive history and endometriosis among premenopausal women. Obstet Gynecol. 2004;104(5 Pt 1):965-74.
- [Google Scholar]
- A retrospective cohort study to evaluate the impact of meaningful weight loss on fertility outcomes in an overweight population with infertility. Fertil Steril. 2014;101:1400-3.
- [Google Scholar]
- A randomized clinical trial to evaluate optimal treatment for unexplained infertility: the fast track and standard treatment (FASTT) trial. Fertil Steril. 2010;94:888-99.
- [Google Scholar]
- The high-sweet-fat food craving among women with premenstrual dysphoric disorder: emotional response, implicit attitude and rewards sensitivity. Psychoneuroendocrinology. 2010;35:1203-12.
- [Google Scholar]
- Six new loci associated with body mass index highlight a neuronal influence on body weight regulation. Nat Genet. 2009;41:25-34.
- [Google Scholar]
- The influence of body weight on response to ovulation induction with gonadotrophins in 335 women with World Health Organization group II anovulatory infertility. BJOG. 2006;113:1195-202.
- [Google Scholar]
- Prevalence of infertility in a cross section of Pakistani population. Pak J Zool. 2010;42:389-93.
- [Google Scholar]
- Polycystic ovary syndrome: a multifaceted disease from adolescence to adult age. Ann N Y Acad Sci. 2006;1092:158-74.
- [Google Scholar]
- Effect of overweight and obesity on assisted reproductive technology − a systematic review. Hum Reprod Update. 2007;13:433-44.
- [Google Scholar]
- Iron status of premenopausal women in a Nigerian University Community. Asian J Clin Nutr. 2010;2:101-7.
- [Google Scholar]
- Effect of maternal height and weight on risk for preterm singleton and twin births resulting from IVF in the United States, 2008-2010. Am J Obstet Gynecol. 2013;209:349e1-6.
- [Google Scholar]
- Endometrial gene expression in the window of implantation is altered in obese women especially in association with polycystic ovary syndrome. Fertil Steril. 2011;95:2335-44.
- [Google Scholar]
- Maternal overweight and obesity and the risk of congenital anomalies: a systematic review and meta-analysis. JAMA. 2009;301:636-50.
- [Google Scholar]
- Obesity reduces uterine receptivity: clinical experience from 9,587 first cycles of ovum donation with normal weight donors. Fertil Steril. 2013;100:1050-8.
- [Google Scholar]
- Obesity at age 20 and the risk of miscarriages, irregular periods and reported problems of becoming pregnant: the Adventist Health Study-2. Eur J Epidemiol. 2012;27:923-31.
- [Google Scholar]
- Overweight women with polycystic ovary syndrome have evidence of subclinical cardiovascular disease. J Clin Endocrinol Metab. 2005;90:5711-6.
- [Google Scholar]
- The impact of maternal body mass index on in vitro fertilization outcomes. J Obstet Gynaecol Can. 2014;36:613-9.
- [Google Scholar]
- Insulin-like growth factor 1 (IGF1), IGF binding protein 3 (IGFBP3), and breast cancer risk: pooled individual data analysis of 17 prospective studies. Lancet Oncol. 2010;11:530-42.
- [Google Scholar]
- Menstrual irregularity and bone mass in premenopausal women: cross-sectional associations with testosterone and SHBG. BMC Musculoskelet Disord. 2010;11:288.
- [Google Scholar]
- The utility of menstrual cycle length as an indicator of cumulative hormonal exposure. J Clin Endocrinol Metab. 2012;97:E1871-9.
- [Google Scholar]
- Age at menarche and risk of ovarian cancer: a meta-analysis of epidemiological studies. Int J Cancer. 2013;132:2894-900.
- [Google Scholar]
- Nicotinic receptor-mediated effects on appetite and food intake. J Neurobiol. 2012;53:618-32.
- [Google Scholar]
- Do quitters have anything to lose? Changes in body mass index for daily, never, and former smokers over an 11-year period (1990–2001) Scand J Public Health. 2009;37:774-7.
- [Google Scholar]
- Cigarette smoking, body mass index, and physical fitness changes among male navy personnel. Nicotine Tob Res. 2011;13:965-71.
- [Google Scholar]
- Gender, smoking and weight concerns: relationship to self-reported body mass index (BMI) Przegl Lek. 2010;67:826-9.
- [Google Scholar]
- The length of perimenopausal menstrual cycles increases later and to a greater degree than previously reported. Fertil Steril. 2006;86:619-24.
- [Google Scholar]
- Menstruation and the menopausal transition. Obstet Gynecol Clin North Am. 2011;38:595-607.
- [Google Scholar]
- Cross-sectional and longitudinal associations between body mass index and marriage-related factors. Obes Res. 2002;10:809-15.
- [Google Scholar]
- Association between menstrual cycle irregularities and endocrine and metabolic characteristics of the polycystic ovary syndrome. Eur J Endocrinol. 2013;168:145-52.
- [Google Scholar]
- The economic impact of obesity in the United States. Diabetes Metab Syndr Obes. 2010;3:285-95.
- [Google Scholar]




